Free Activity Parq PDF Template
Free Activity Parq PDF Template
In the realm of public health and personal fitness, the significance of assessing one’s readiness for physical activity cannot be overstated. A cornerstone tool in this assessment is the 2021 Physical Activity Readiness Questionnaire for Everyone (PAR-Q+), designed to discern the safety of engaging in physical activity for individuals considering an increase in their level of physical exertion. The PAR-Q+ is grounded in the premise that while the health benefits of regular physical activity are manifold and well-documented, ensuring that such activity is undertaken safely is paramount, especially for those with underlying health conditions. Through a series of meticulously crafted questions, the form aids individuals in evaluating potential risks and the need for medical consultation before embarking on or enhancing their physical activity routine. This questionnaire covers a wide range of health conditions including, but not limited to, heart conditions, chest pain, balance issues, chronic medical conditions, medication use, joint or soft tissue concerns, and other conditions that might be exacerbated by increased physical activity. Furthermore, it incorporates follow-up questions on specific medical conditions, providing a comprehensive health screening tool. Significantly, the PAR-Q+ also serves as a declaration of understanding and acceptance of risk by the participant, underscoring the critical role personal responsibility plays in health and fitness endeavors. By meticulously guiding individuals through their current health status and potential risks associated with increased physical activity, the PAR-Q+ embodies a proactive approach to health promotion and disease prevention.
2021
The Physical Activity Readiness Questionnaire for Everyone
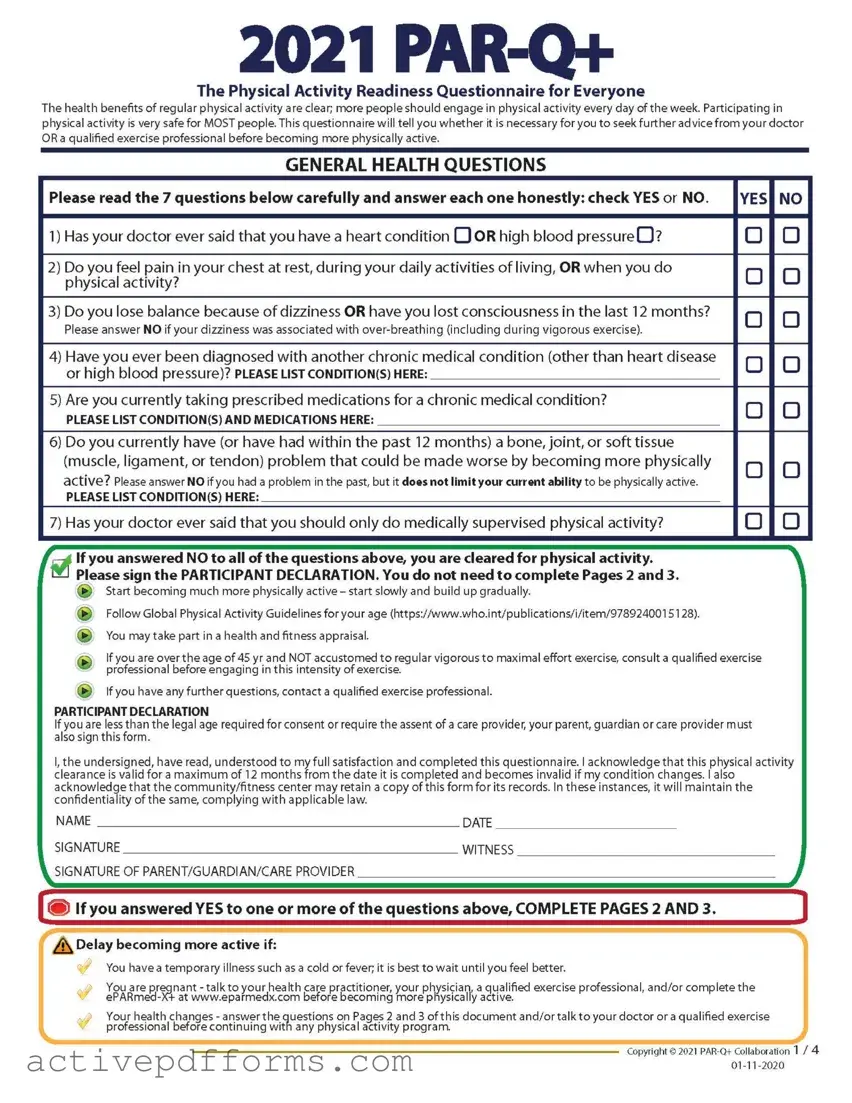
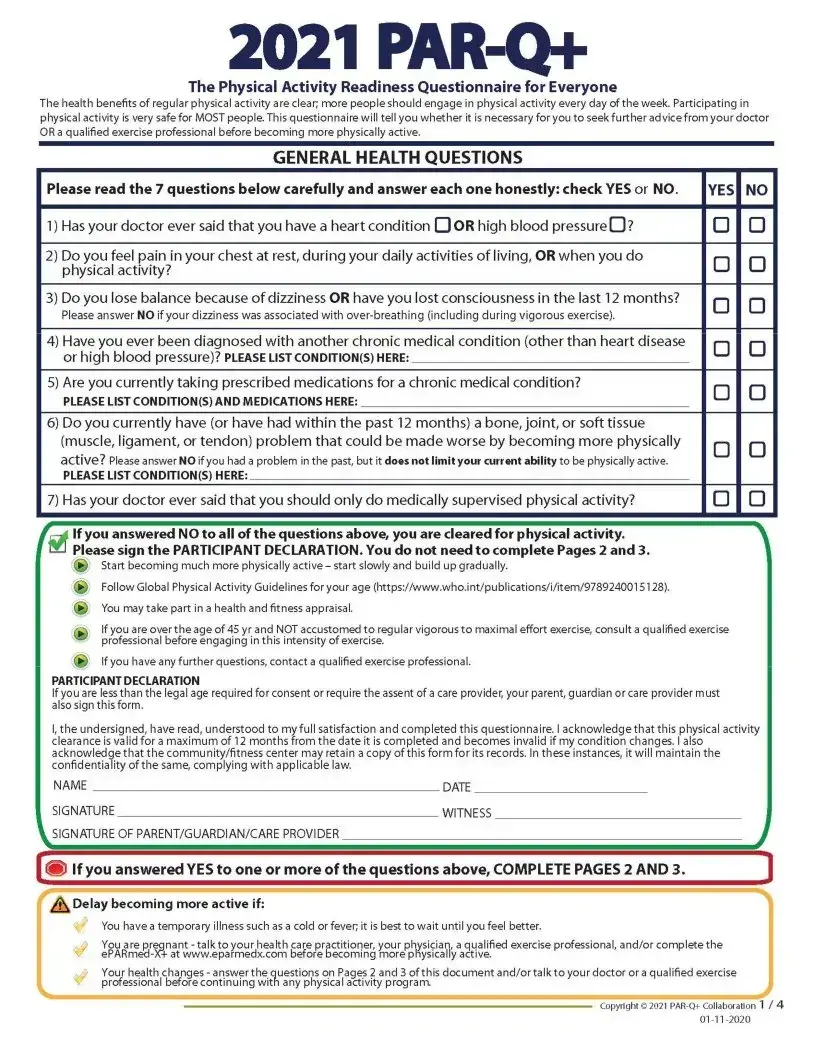
The health benefits of regular physical activity are clear; more people should engage in physical activity every day of the week. Participating in physical activity is very safe for MOST people. This questionnaire will tell you whether it is necessary for you to seek further advice from your doctor OR a qualified exercise professional before becoming more physically active.
GENERAL HEALTH QUESTIONS
Please read the 7 questions below carefully and answer each one honestly: check YES or NO. |
YES NO |
1)Has your doctor ever said that you have a heart condition OOR high blood pressure O?
2)Do you feel pain in your chest at rest, during your daily activities of living, OR when you do physical activity?
3)Do you lose balance because of dizziness OR have you lost consciousness in the last 12 months?
Please answer NO if your dizziness was associated with
4)Have you ever been diagnosed with another chronic medical condition (other than heart disease or high blood pressure)? please listcondition(S) here:
5)Are you currently taking prescribed medications for a chronic medical condition?
PLEASE LIST CONDITION(S) AND MEDICATIONS HERE:
6)Do you currently have (or have had within the past 12 months) a bone, joint, or soft tissue (muscle, ligament, or tendon) problem that could be made worse by becoming more physically
active? Please answer NO if you had a problem in the past, but it doesnot limit your current ability to be physically active.
PLEASE LIST CONDITION(S) HERE:
o
o
7) Has your doctor ever said that you should only do medically supervised physical activity?
If you answered NO to all of the questions above, you are cleared for physical activity.
Start becoming much more physically active - start slowly and build up gradually.
Follow Global Physical Activity Guidelines for your age (https://www.who.int/publications/i/item/9789240015128).
You may take part in a health and fitness appraisal.
If you are over the age of 45 yr and NOT accustomed to regular vigorous to maximal effort exercise, consult a qualified exercise professional before engaging in this intensity of exercise.
►If you have any further questions, contact a qualified exercise professional.
PARTICIPANT DECLARATION
If you are less than the legal age required for consent or require the assent of a care provider, your parent, guardian or care provider must also sign this form.
I, the undersigned, have read, understood to my full satisfaction and completed this questionnaire. I acknowledge that this physical activity clearance is valid for a maximum of 12 months from the date it is completed and becomes invalid if my condition changes. I also acknowledge that the community/fitness center may retain a copy of this form for its records. In these instances, it will maintain the confidentiality of the same, complying with applicable law.
NAME |
DATE |
SIGNATURE _____________________________________ |
WITNESS |
SIGNATURE OF PARENT/GUARDIAN/CARE PROVIDER |
|
[i® If you answered YES to one or more of the questions above, COMPLETE PAGES 2 AND 3.
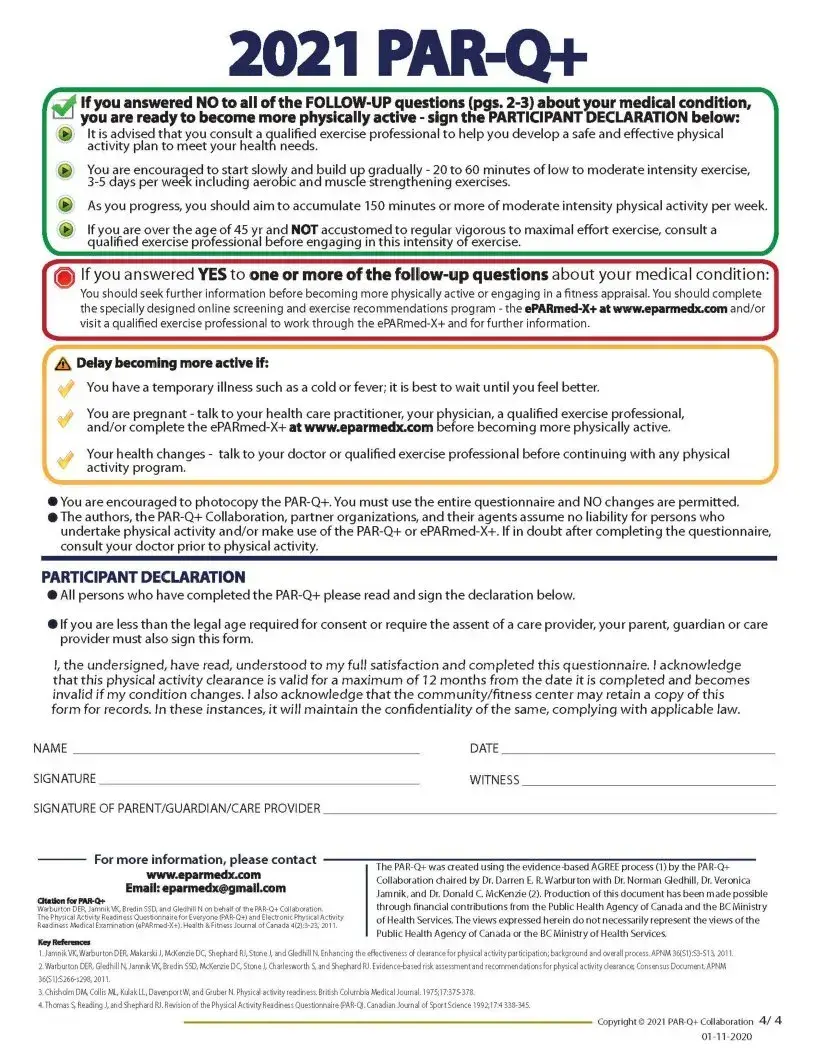
/*\ Delay becoming more active if:
You have a temporary illness such as a cold orfever; it is best to wait until you feel better.
You are pregnant - talk to your health care practitioner, your physician, a qualified exercise professional, and/or complete the
Your health changes - answer the questions on Pages 2 and 3 of this document and/ortalkto your doctor ora qualified exercise professional before continuing with any physical activity program.
J
3
2021
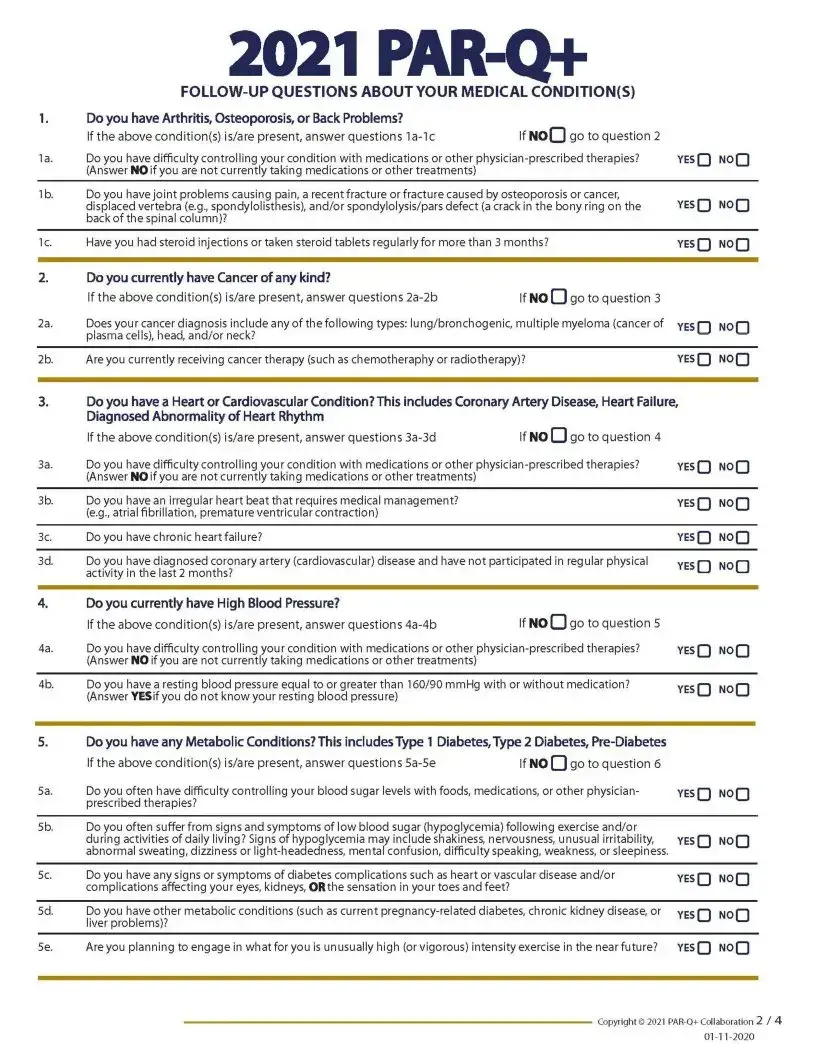
1.Do you have Arthritis, Osteoporosis, or Back Problems?
|
If the above condition(s) is/are present, answer questions |
If noQ go to question 2 |
|
la. |
Do you have difficulty control ling your condition with medications or other |
yesQ NOQ |
|
|
(Answer NO if you are not currently taking medications or other treatments) |
|
|
lb. |
Do you have joint problems causing pain, a recent fracture or fracture caused by osteoporosis or cancer, |
YESQ NOQ |
|
|
displaced vertebra (e.g., spondylolisthesis), and/or spondylolysis/pars defect (a crack in the bony ring on the |
||
|
back of the spinal column)? |
|
|
1c. |
Have you had steroid injections or taken steroid tablets regularly for more than 3 months? |
YESQ NOQ |
|
2.Do you currently have Cancer of any kind?
|
If the above condition(s) is/are present, answer questions |
If NO O go to question 3 |
|
2a. |
Does your cancer diagnosis include any of the following types: lung/bronchogenic, multiple myeloma (cancer of |
yes[“) NO |
|
|
plasma cells), head, and/or neck? |
|
u |
2b. |
Are you currently receiving cancer therapy (such as chemotheraphy or radiotherapy)? |
YESQ NOQ |
|
3.Do you have a Heart or Cardiovascular Condition? This includes Coronary Artery Disease, Heart Failure, Diagnosed Abnormality of Heart Rhythm
If the above condition(s) is/are present, answer questions |
If NO |
go to question 4 |
3a. Do you have difficulty controlling your condition with medications or other
3 b. Do you have an irregular heart beat that requires medical management? (e.g., atrial fibrillation, premature ventricular contraction)
3c. Do you have chronic heart failure?
3d. Do you have diagnosed coronary artery (cardiovascular) disease and have not participated in regular physical activity in the last 2 months?
4. |
Do you currently have High Blood Pressure? |
|
|
If the above condition(s) is/are present, answer questions |
If NO O 9° to question 5 |
4a. |
Do you have difficulty controlling your condition with medications or other |
|
|
(Answer NO if you are not currently taking medications or other treatments) |
|
4b. |
Do you have a resting blood pressure equal to or greater than 160/90 mmHg with or without medication? |
|
|
(Answer YES if you do not know your resting blood pressure) |
|
YESQ NOQ
yesQ NOQ
yesQ NOQ
YESQ NOQ
yesQ NOQ
YESQ NOQ
5.Do you have any Metabolic Conditions? This includes Type 1 Diabetes,Type 2 Diabetes,
|
If the above condition(s) is/are present, answer questions |
If NO [~] go to question 6 |
|
|
5a. |
Do you often have difficulty controlling your blood sugar levels with foods, medications, or other physician- |
YESQ |
NOQ |
|
|
prescribed therapies? |
|
|
|
5 b. |
Do you often suffer from signs and symptoms of low blood sugar (hypoglycemia) following exercise and/or |
|
|
|
|
during activities of daily living? Signs of hypoglycemia may include shakiness, nervousness, unusual irritability, |
YESQ |
NOQ |
|
abnormal sweating, dizziness or
5c. |
Do you have any signs or symptoms of diabetes complications such as heart or vascular disease and/or |
YESQ NOQ |
|
complications affecting your eyes, kidneys, ORthe sensation in your toes and feet? |
|
5d. Do you have other metabolic conditions (such as current
5e. Are you planning to engage in what for you is unusually high (or vigorous) intensity exercise in the near future?
<- VI |
NOQ |
in □ |
|
YESQ NOQ
2021
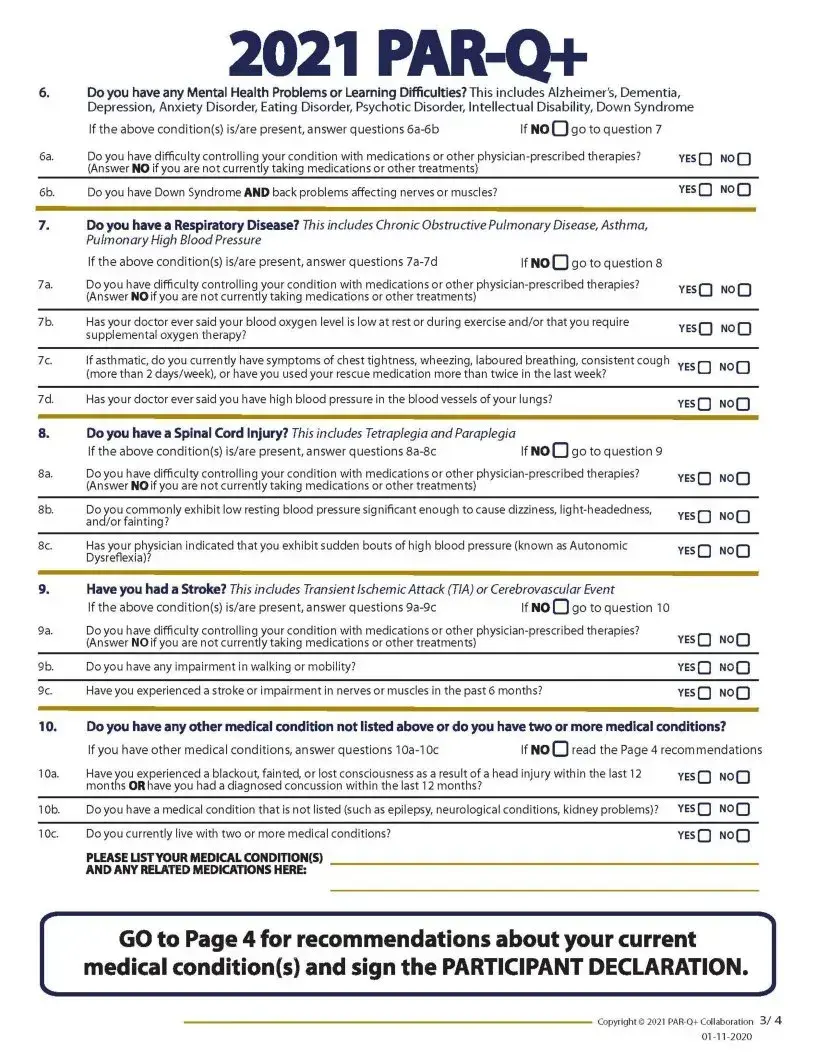
6.Do you have any Mental Health Problems or Learning Difficulties? This includes Alzheimer's, Dementia, Depression, Anxiety Disorder, Eating Disorder, Psychotic Disorder, Intellectual Disability, Down Syndrome
|
If the above condition(s) is/are present, answer questions |
If NO O go to question 7 |
|
6a. |
Do you have difficulty controlling your condition with medications or other |
yesQ NOQ |
|
|
(Answer NO if you are not currently taking medications or other treatments) |
|
|
6b. |
Do you have Down Syndrome AND back problems affecting nerves or muscles? |
|
yesQ NOQ |
7.Do you have a Respiratory Disease? This includes Chronic Obstructive Pulmonary Disease, Asthma, Pulmonary High Blood Pressure
If the above condition(s) is/are present, answer questions |
|f NO Q go to question 8 |
7a. Do you have difficulty controlling your condition with medications or other
7 b. Has your doctor ever said your blood oxygen level is low at rest or during exercise and/or that you require supplemental oxygen therapy?
7c. If asthmatic, do you currently have symptoms of chest tightness, wheezing, laboured breathing, consistent cough (more than 2 days/week), or have you used your rescue medication more than twice in the last week?
7d. Has your doctor ever said you have high blood pressure in the blood vessels of your lungs?
8.Do you have a Spinal Cord Injury? This includes Tetraplegia and Paraplegia
If the above condition(s) is/are present, answer questions |
If NO O go to question 9 |
8a. Do you have difficulty controlling your condition with medications or other
8 b. Do you commonly exhibit low resting blood pressure significant enough to cause dizziness,
8c. Has your physician indicated that you exhibit sudden bouts of high blood pressure (known as Autonomic Dysreflexia)?
9.Have you had a Stroke? This includes Transient Ischemic Attack (TIA) or Cerebrovascular Event
If the above condition(s) is/are present, answer questions |
If NO Q go to question 10 |
9a. Do you have difficulty controlling your condition with medications or other
9 b. Do you have any impairment in walking or mobility?
9c. Have you experienced a stroke or impairment in nerves or muscles in the past 6 months?
YESQ noQ
yesQ noQ
yesQ NOQ
YESQ NoQ
yesQ NoQ
yesQ NOQ
yesQ noQ
yesQ NOQ
yesQ NOQ
YESQ NOQ
10.Do you have any other medical condition not listed above or do you have two or more medical conditions?
|
If you have other medical conditions, answer questions |
If NqQ read the Page 4 recommendations |
||
10a. |
Have you experienced a blackout, fainted, or lost consciousness as a result of a head injury within the last 12 |
YESQ |
NOQ |
|
|
months OR have you had a diagnosed concussion within the last 12 months? |
|
|
|
10b. |
Do you have a medical condition that is not listed (such as epilepsy, neurological conditions, kidney problems)? |
YESQ |
NoQ |
|
10c. |
Do you currently live with two or more medical conditions? |
|
YESQ |
NOQ |
|
PLEASE LISTYOUR MEDICAL CONDITION(S) |
|
|
|
|
AND ANY RELATED MEDICATIONS HERE: |
|
|
|
GO to Page 4 for recommendations about your current medical condition(s) and sign the PARTICIPANT DECLARATION.
2021
You have a temporary illness such as a cold or fever; it is best to wait until you feel better.
You are pregnant - talk to your health care practitioner, your physician, a qualified exercise professional,
and/or complete the
Your health changes - talk to your doctor or qualified exercise professional before continuing with any physical activity program.
•You are encouraged to photocopy the
•The authors, the
PARTICIPANT DECLARATION
•All persons who have completed the
•If you are less than the legal age required for consent or require the assent of a care provider, your parent, guardian or care provider must also sign this form.
I, the undersigned, have read, understood to my full satisfaction and completed this questionnaire. I acknowledge that this physical activity clearance is valid for a maximum of 12 months from the date it is completed and becomes invalid if my condition changes. I also acknowledge that the community/fitness center may retain a copy of this form for records. In these instances, it will maintain the confidentiality of the same, complying with applicable law.
NAME
SIGNATURE
SIGNATURE OF PARENT/GUARDIAN/CARE PROVIDER
www.eparmedx.com
Email: eparmedx^gmailxom
Otttfcn for
Warburton DER, Jamnik VK, Bred in SSD, and Gledhill N on behalf of the
The Physical Activity Readiness Questionnaire for Everyone
Key Referanees
DATE
WITNESS
The
Collaboration chaired by Dr. Darren E. R. Warburton with Dr. Norman Gledhill, Dr. Veronica Jamnik,and Dr. Donald C. McKenzie (2). Production of this document has been made possible through financial contributions from the Public Health Agency of Canada and the BC Ministry of Health Services. The views expressed herein do not necessarily represent the views of the
Public Health Agency of Canada or the BC Ministry of Health Services.
1.Jamnik VK, Warburton DER, Makarski J, McKenzie DC, Shephard RJ, Stone J, and Gledhill N. Enhancing the effectiveness of clearance for physical activity participation; background and overall process. APNM
2.Warburton DER, Gledhill N,JamnikVK, Bredin SSD, McKenzie DC, Stone J, Charlesworth S, and Shephard RJ.
3.Chisholm DM, Collis ML, Kulak LL, DavenportW, and Gruber N. Physical activity readiness. British Columbia Medical Journal.
4.Thomas S, Reading J, and Shephard RJ. Revision of the Physical Activity Rea din ess Questionnaire
01
| Fact Name | Detail |
|---|---|
| Form Purpose | The 2021 PAR-Q+ is designed to determine the safety of physical activity for individuals. |
| Target Audience | Intended for EVERYONE looking to become more physically active. |
| Health Benefits Highlight | Emphasizes the clear health benefits of regular physical activity. |
| Safety Assurance | Participating in physical activity is very safe for MOST people. |
| Health Questions | Contains seven general health questions that must be answered honestly with YES or NO. |
| Follow-up Actions | Guides individuals on next steps based on their questionnaire responses. |
| Participant Declaration | Requires a signature to acknowledge understanding and completeness of the form. |
| Validity Period | The clearance provided by the form is valid for a maximum of 12 months from completion. |
| Record Confidentiality | Assures that any retained copy of the form will be kept confidential, complying with applicable law. |
Filling out the Activity PAR-Q form is an important step for anyone looking to become more physically active, especially if health issues are a concern. This questionnaire helps determine if you should seek advice from a doctor or a qualified exercise professional before increasing your activity levels. Following the steps detailed below ensures that the form is completed accurately, which is crucial for your safety and health.
Once you have completed all steps and filled out the form accurately, you are ready to discuss your physical activity plans with a professional if necessary. Remember, this form is a tool to help ensure your safety and health as you become more physically active. Keep a copy for your records and respect the privacy and confidentiality of the information provided.
What is the PAR-Q+ form?
The Physical Activity Readiness Questionnaire for Everyone (PAR-Q+) is a tool designed to help individuals determine whether they need to seek advice from a doctor or a qualified exercise professional before starting to become more physically active. It aims to ensure safety during physical activity by identifying any potential health risks.
Why should I complete the PAR-Q+ form?
Completing the PAR-Q+ form is crucial because it helps you identify any health issues that could make physical activity unsafe for you. By recognizing these issues early, you can get proper advice on how to safely engage in physical activities, thereby maximizing the health benefits while minimizing the risks.
How often should I complete the PAR-Q+ form?
The PAR-Q+ form should be completed at least once every 12 months or whenever your health condition changes. This timeframe ensures that the information stays current, reflecting any new health concerns or changes in your physical condition that could impact your ability to safely engage in physical activity.
What happens if I answer "YES" to any questions on the PAR-Q+ form?
If you answer "YES" to any of the questions, you should complete the follow-up questions on Pages 2 and 3 of the document. These questions provide more detailed inquiries about specific medical conditions. Based on your answers, you may be advised to consult a doctor or a qualified exercise professional before becoming more physically active.
Can I still exercise if I answer "YES" to any of the questions on the PAR-Q+ form?
Yes, but you may need to modify your exercise plan based on professional advice. Answering "YES" to any question on the PAR-Q+ form does not automatically disqualify you from physical activity. Instead, it indicates that you should seek further advice to ensure your exercise plan is safe and tailored to your specific health conditions.
What if my health condition changes after I’ve completed the PAR-Q+ form?
If your health condition changes after completing the PAR-Q+ form, it is important to re-assess your readiness for physical activity. Changes in your health can impact the safety and benefits of exercise for you, so updating your PAR-Q+ responses and consulting with a healthcare professional are recommended steps before continuing or adjusting your physical activity plan.
Is the information I provide on the PAR-Q+ form confidential?
Yes, the information you provide on the PAR-Q+ form is confidential. Organizations that collect this information are required to maintain its confidentiality, complying with applicable law to ensure your personal health information is protected.
Do I need a doctor’s note to start exercising if I answer "NO" to all the questions on the PAR-Q+ form?
If you answer "NO" to all the questions, generally, you do not need a doctor's note to start exercising. This indicates that you are likely at a low risk for complications from physical activity. However, it's essential to start slowly and build up gradually, following global physical activity guidelines for your age group.
What are the next steps after completing the PAR-Q+ form?
If you answered "NO" to all questions, you are cleared to become more physically active - starting with activities that match your current fitness level and gradually increasing intensity. If you answered "YES" to any questions, follow the next steps detailed on Pages 2 and 3 of the form, which may include consulting with a healthcare provider or an exercise professional.
Where can I find more information or get help with the PAR-Q+ form?
For more information or assistance with the PAR-Q+ form, you are encouraged to contact a qualified exercise professional or visit the official ePARmed-X+ website at www.eparmedx.com. This website offers additional resources and guidance for safely increasing physical activity levels.
When completing the Physical Activity Readiness Questionnaire (PAR-Q+), individuals often make mistakes that can affect the accuracy and usefulness of the form. Recognizing and avoiding these common errors can help ensure that the information provided is reliable and that the subsequent advice regarding physical activity is appropriate. Here are four common mistakes:
Not reading the questions thoroughly: Given the importance of each question in assessing health risks related to physical activity, skimming over them too quickly or not paying close attention to the details can lead to incorrect responses. It's crucial to read each question carefully and consider your health and physical condition comprehensively before answering.
Providing incomplete medical information: When the questionnaire asks for specific medical conditions or medications, some people might omit details either unintentionally or due to privacy concerns. However, withholding this information can prevent the questionnaire from providing accurate activity recommendations, potentially increasing the risk of injury or adverse health effects.
Overlooking the importance of accurately listing symptoms: If you experience symptoms such as dizziness, chest pain, or loss of balance, it's essential to mention these in the questionnaire. Some individuals might not consider these symptoms significant or may forget to include them if they don't occur frequently, but they can be crucial indicators of underlying health issues that need to be considered when planning physical activity.
Ignoring the need for professional advice: The questionnaire clearly states when it's necessary to seek further advice from a doctor or a qualified exercise professional before becoming more physically active. Some people might disregard this recommendation, especially if they feel capable or are eager to start a new fitness regime. However, bypassing professional consultation can overlook potential health risks that could be mitigated with proper guidance.
By paying close attention to each of these potential mistakes and taking the time to answer thoughtfully and accurately, individuals can maximize the benefit of the PAR-Q+ and engage in physical activities that are safe and beneficial for their health conditions.
When individuals are preparing to increase their physical activity levels or start a new exercise program, the Physical Activity Readiness Questionnaire (PAR-Q+) is a critical first step in ensuring safety and readiness for physical exertion. However, the PAR-Q+ is often accompanied by other forms and documents that help create a comprehensive overview of a person's health and fitness level. These additional documents can provide in-depth insights and create a safer, more tailored exercise regimen.
These documents, together with the PAR-Q+, form a comprehensive toolkit for assessing individuals' readiness and creating a balanced, safe, and personalized exercise program. Each document serves a unique purpose, ensuring that all health, safety, and personal preferences are accounted for before starting or modifying a physical activity regimen. This multifaceted approach contributes to the overall success and sustainability of a health and fitness journey.
The Medical History Form commonly used in health care settings shares similarities with the Activity PAR-Q form as both collect detailed health information to identify any potential risks before undertaking a new activity or treatment.
A Consent Form for Physical Activity Programs is similar because it involves the participant acknowledging the risks associated with physical activity and their understanding of those risks, much like the participant declaration in the Activity PAR-Q form.
The Pre-Participation Physical Evaluation often required for school or sports activities resembles the Activity PAR-Q form. They both assess an individual's readiness for physical activity and identify any conditions that might limit participation.
Emergency Contact Information Forms have a similarity in that they are both preparative documents designed to ensure safety in different environments; the PAR-Q by assessing health risks, and emergency forms by providing contact information in case of an incident.
Risk Assessment Forms used in workplaces to evaluate potential hazards that employees might face is conceptually similar to the Activity PAR-Q form's purpose of assessing health risks before engaging in physical activity.
Health Screening Questionnaires used by health organizations to screen for diseases have a similar application as the Activity PAR-Q form, with both aiming to identify health issues that may be exacerbated by new or increased levels of activity.
A Drug and Allergy Interactions Form used in pharmaceutical settings is similar because, like the Activity PAR-Q form, it helps identify conditions (in this case, potential drug and allergy interactions) that require caution or adjustments in approach.
The Physical Activity Guidelines provided by various health authorities share a goal with the Activity PAR-Q form—they both aim to guide individuals towards safe and appropriate levels of physical activity based on their current health status and age.
When filling out the Activity PAR-Q form, it's crucial to follow guidelines that ensure accuracy and safety. Here are some dos and don'ts to consider:
Do:Many people hold misconceptions about the Physical Activity Readiness Questionnaire (PAR-Q+). It is important to clarify these misunderstandings to ensure everyone can safely engage in physical activity. Here are eight common misconceptions:
This is not true. The PAR-Q+ is designed for individuals of all ages who are looking to become more physically active. It helps assess readiness for physical activity and identifies those who may need further medical advice.
This is a misconception. The PAR-Q+ is a self-screening tool to determine if you should consult a healthcare professional before starting an exercise program. It does not replace a comprehensive medical examination.
Even if you feel healthy, completing the PAR-Q+ can identify potential risks associated with increased physical activity that might not be obvious to you.
The truth is, your health status can change, making it necessary to complete the PAR-Q+ at least once every 12 months or sooner if your health changes.
Not necessarily. If you answer "Yes" to any questions, it means you should seek further advice from a doctor or qualified exercise professional before increasing your physical activity levels, not that you must avoid exercise altogether.
While some situations may require visiting a doctor, others might only need advice from a qualified exercise professional who can suggest appropriate ways to safely engage in physical activity.
The questionnaire is designed to be user-friendly. It consists of simple yes or no questions about your health and guides you whether to seek further advice before becoming more active.
This is incorrect. Signing the declaration acknowledges you’ve honestly answered the questions and understand your current physical activity readiness. It does not mean you waive rights in case of injury resulting from exercise.
Understanding the purpose and process of the PAR-Q+ can help individuals safely increase their physical activity levels. It’s an important step in ensuring the safety and health of everyone looking to become more active.
Filling out and using the Activity PAR-Q (Physical Activity Readiness Questionnaire) form is an essential step for individuals planning to increase their level of physical activity, especially if they have existing health concerns or conditions. Here are key takeaways from the 2021 PAR-Q+ document:
Using the Activity PAR-Q+ form responsibly supports safe participation in physical activities, especially for individuals with existing health conditions or those with specific health-related queries. It serves as a critical tool in promoting health and wellness through safe physical activity participation.
Filing a Motion in Family Court - Provides a guided framework for individuals seeking to make legal adjustments to family orders without the need for extensive legal jargon.
Vehicle Registration Va - Guidelines on the legal requirement to notify the Virginia DMV about changes to vehicle registration details.
Cuddy Buddy Application - Embrace the therapeutic effects of human touch, scientifically proven to reduce stress and increase happiness, by applying for a cuddle buddy today.