Free Annual Physical Examination PDF Template
Free Annual Physical Examination PDF Template
The Annual Physical Examination form is an integral component in the health management process, designed meticulously to gather comprehensive health information from an individual to ensure personalized and thorough medical care. Before stepping into the doctor's office, patients are required to fill out this extensive form that covers several vital sections. The initial part of the form is dedicated to personal information, including name, date of birth, sex, social security number, and contact details, setting the foundation for the examination. A crucial segment that follows outlines diagnoses or significant health conditions, current medications along with dosage, frequency, and prescribing physician—which necessitates an additional page if the list is extensive—and allergies or medication sensitivities. Key immunization records, such as Tetanus/Diphtheria, Hepatitis B, Influenza, and Pneumovax, alongside TB screening results and a statement about communicable diseases, form another significant component, ensuring individual and public health safety. The form navigates through past medical interventions including hospitalizations and surgical procedures, shedding light on the patient’s medical history. The second part delves into the general physical examination, recording vital signs, evaluation of body systems, vision and hearing screenings, with a provision for additional comments to capture any changes or special recommendations post-consultation. Detailed recommendations for health maintenance, potential activity restrictions, use of adaptive equipment, and adjustments in health status from the previous year are solicited for a holistic understanding. This form acts as a conduit for communication between the patient and medical professionals, streamlining the process for an efficient and effective annual physical examination.
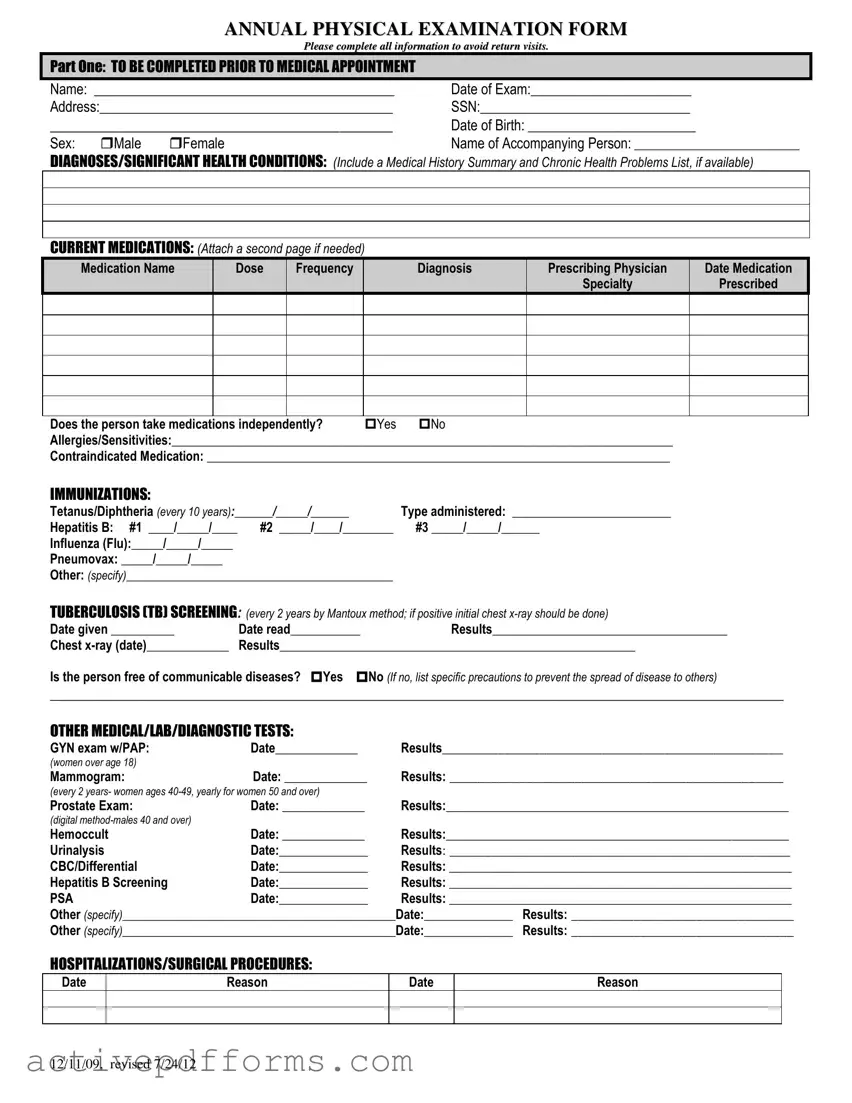
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
| Fact Name | Detail |
|---|---|
| Form Purpose | This form is used for documenting an individual's Annual Physical Examination. |
| Completion Requirement | All information must be completed to avoid return visits. |
| Part One: Information | To be filled out prior to the medical appointment, including personal and medical history information. |
| Documentation of Medications | Details of current medications including dose, frequency, and prescribing physician must be attached. |
| Immunization and Screenings | Records of immunizations and screenings like Tetanus/Diphtheria, Hepatitis B, Influenza, and Tuberculosis (TB) are required. |
| Part Two: Examination Outcomes | Includes blood pressure, pulse, temperature, and evaluation of systems such as cardiovascular, respiratory, and more. |
| Governing Law(s) | Specific requirements may vary by state, but generally adhere to federal guidelines for health records privacy. |
Filling out the Annual Physical Examination form is a meticulous process that ensures your medical records are up to date and provides a comprehensive overview of your current health status. This step-by-step guide aims to help you complete the form accurately, avoiding the need for return visits due to missing or incorrect information. By carefully providing all the necessary details, you ensure that healthcare providers have the information they need to offer the best care possible.
Once the form is fully completed, review it to ensure accuracy before submitting it to the required medical facility or healthcare provider. This detailed form is a vital tool in managing the patient's care, making accurate completion crucial for optimal healthcare outcomes.
What is the purpose of the Annual Physical Examination Form?
This form serves as a comprehensive record for patients undergoing an annual physical examination. It ensures that all relevant personal, medical, and diagnostic information is systematically captured and updated. This facilitates effective monitoring of the patient's health status, aids in the early detection of any health issues, and supports ongoing management of existing conditions.
Who needs to complete the Annual Physical Examination Form?
Patients seeking to undergo their yearly physical check-up are required to fill out this form. Part one of the form is to be completed by the patient or the accompanying person prior to the medical appointment. The healthcare provider completes part two during the examination, summarizing findings and recommendations.
What information is required in Part One of the form?
Part One collects personal details, including the patient's name, date of examination, address, Social Security Number (SSN), date of birth, and sex. It also requires medical history, listing diagnoses/significant health conditions, current medications, allergies or sensitivities, immunization records, tuberculosis (TB) screenings, and details regarding previous hospitalizations or surgical procedures.
What happens if information is missing from the form?
Leaving sections incomplete may necessitate return visits to provide the missing information, delaying the examination process and proper follow-up care. It's crucial to fill out all requested details accurately to avoid any inconvenience and ensure comprehensive evaluation and care.
Can additional pages be attached to the form?
Yes, if the space provided for certain sections like current medications is insufficient, additional pages can be attached to the form. It's important to clearly mark these pages with the patient's name and attach them securely to avoid misplacement or confusion.
How often should the Tetanus/Diphtheria immunization and TB screening be updated?
The Tetanus/Diphtheria immunization is recommended every 10 years, while the TB screening needs to be conducted every 2 years using the Mantoux method. If the initial TB test is positive, a follow-up chest x-ray should be done to further assess the patient's condition.
What diagnostic tests are included in Part One?
The form lists several diagnostic tests such as GYN exams with PAP smears, mammograms, prostate exams, Hemoccult tests for blood in stool, urinalysis, complete blood count (CBC), Hepatitis B screening, and prostate-specific antigen (PSA) tests, among others. Dates and results of these tests need to be recorded, as they provide critical information about the patient's health.
What does Part Two of the form entail?
Part Two focuses on the general physical examination conducted by the healthcare provider. It covers blood pressure, pulse, respirations, temperature, height, weight, and an evaluation of various body systems. It also includes sections for vision and hearing screenings, additional comments, medication adjustments, health maintenance recommendations, dietary instructions, emergency treatment information, activity limitations, adaptive equipment use, health status changes, and recommended specialty consults.
Is it necessary for the physician to sign the form?
Absolutely. The physician's signature, along with their printed name, date, address, and phone number, is required to validate the form. This authentication confirms that the examination was performed, and the information recorded is accurate to the best of the physician's knowledge and belief.
The process of completing an Annual Physical Examination form is critical for ensuring accurate medical evaluation and care. Yet, individuals frequently make mistakes that can lead to complications or misinterpretations of their health status. Identifying and understanding these common errors can greatly improve the quality of information provided to healthcare professionals. Below are eight critical mistakes to be aware of:
Omitting personal information, such as name, date of birth, or Social Security Number, which is essential for patient identification and record keeping.
Failure to list diagnoses or significant health conditions accurately. This section provides healthcare providers with a snapshot of the patient's medical history, and overlooking details can lead to inadequate care planning.
Improper documentation of current medications, including dosage, frequency, and purpose. Medication management is a critical component of patient care, and inaccuracies can result in adverse drug interactions or ineffective treatment strategies.
Not specifying allergies or sensitivities, which is crucial for preventing adverse reactions during treatment or medication administration.
Overlooking immunization records. Immunizations protect against specific diseases, and missing entries may lead to unnecessary revaccination or leave the individual unprotected.
Incomplete Tuberculosis (TB) screening information. TB screening is a preventative measure, and missing or outdated information might lead to overlooked infections.
Skipping details of previous hospitalizations or surgical procedures. This information offers insights into past major medical events that could influence current health status and future medical decisions.
Failure to accurately report the results of recent medical/lab/diagnostic tests. These results can indicate the presence of conditions that require immediate attention or long-term management.
By avoiding these common mistakes, individuals can ensure their healthcare providers have the most accurate and comprehensive information, leading to more effective and personalized treatment plans. This not only streamlines the medical appointment process but also enhances the overall standard of care received.
When completing an Annual Physical Examination, it's essential to provide comprehensive healthcare information to ensure accurate evaluation and necessary follow-up care. Alongside the main form, there are additional documents often used to compile a full medical profile. These documents play a crucial role in painting a complete picture of an individual's health status, enhancing the effectiveness of the physical examination. Here are four notable forms and documents typically used in conjunction with the Annual Physical Examination form:
Together, these documents, along with the Annual Physical Examination form, empower healthcare providers to offer personalized, proactive medical care. By having a clear understanding of a patient's comprehensive medical history, current health status, and future care preferences, physicians can make more informed decisions, ultimately leading to better health outcomes for patients.
The Medical History Form closely resembles the Annual Physical Examination form due to its comprehensive collection of past medical information. It gathers data on prior diagnoses, significant health conditions, and a summary of the patient's medical history, crucial for providing context and understanding the patient’s current health status.
The Medication List Form is similar because both documents require detailed information about the patient's current medications, including names, dosages, frequency, and the prescribing physician's details. This comparison emphasizes the importance of maintaining accurate and up-to-date medication records to ensure safe and effective pharmaceutical management.
A Vaccination Record Form shares similarities with the section of the Annual Physical Examination form that records immunizations. Both document the dates and types of vaccines administered, such as Tetanus/Diphtheria, Hepatitis B, Influenza, and others, to track the patient's immunization status and adherence to recommended vaccination schedules.
The Diagnostic Test Results Form is akin to the segment of the Annual Physical Examination form detailing results from tests such as mammograms, prostate exams, urinalysis, and more. This likeness underscores the role of both documents in compiling and assessing diagnostic information crucial for diagnosing, monitoring, and treating various health conditions.
When it comes to filling out an Annual Physical Examination form, it's essential to approach this task with attentiveness and precision. Here are eight key dos and don'ts that will help ensure the process is smooth, and the information provided is accurate and comprehensive.
Remember, this form is a vital tool in managing your healthcare. Providing detailed, accurate, and up-to-date information is crucial for your healthcare provider to offer the best care possible. If you have questions or need assistance, don't hesitate to contact your healthcare provider's office. Your health deserves careful attention.
There are several common misconceptions about the Annual Physical Examination form that require clarification to ensure that patients and their caregivers fully understand the process and its importance. These misconceptions can lead to confusion, missed opportunities for preventative care, and an incomplete understanding of an individual's health status.
While the form begins with sections that should be filled out prior to the medical appointment by the patient or caregiver, it also includes parts that are explicitly meant to be completed by a healthcare provider during the examination. This division is designed to gather comprehensive information from both the patient and the medical evaluation.
The form serves not only to document any new diagnoses or health concerns but also includes a thorough review of the patient's existing conditions, medication, allergies, immunization records, and previous diagnostic tests. This holistic view supports ongoing health management and preventative care strategies.
Adult immunization records play a crucial role in preventative health. Up-to-date vaccinations are essential not just for children but for adults as well, to protect against diseases such as tetanus, diphtheria, influenza, and pneumococcal infections. This section of the form should be completed to ensure all immunizations are current.
Even if there are no perceived changes in health, it is vital to complete the form annually. This regular update allows for the monitoring of potential subtle changes in health status over time, ensuring continuity in care and the opportunity for early intervention when necessary.
Clarifying these misconceptions reinforces the value of the Annual Physical Examination form as a fundamental tool in managing and maintaining optimal health through preventative care and comprehensive medical review.
Filling out an Annual Physical Examination form is a critical task that ensures your healthcare providers have all the necessary information to offer the best care possible. Here are key takeaways to consider while filling out and using this form:
By accurately filling out and updating the Annual Physical Examination form, you ensure that your healthcare team has all the essential information to provide personalized and effective care. Remember, this form is not only a record but a crucial tool in managing your health and wellness journey.
Sample Church Demographics Form - The form is designed to ensure all necessary demographic and contact information is readily available for healthcare providers.
Florida Proof Loss - Providing a legal framework, this form aids in reporting property loss claims, emphasizing the significance of transparency for a fair settlement.