Free Caregiver Daily Log PDF Template
Free Caregiver Daily Log PDF Template
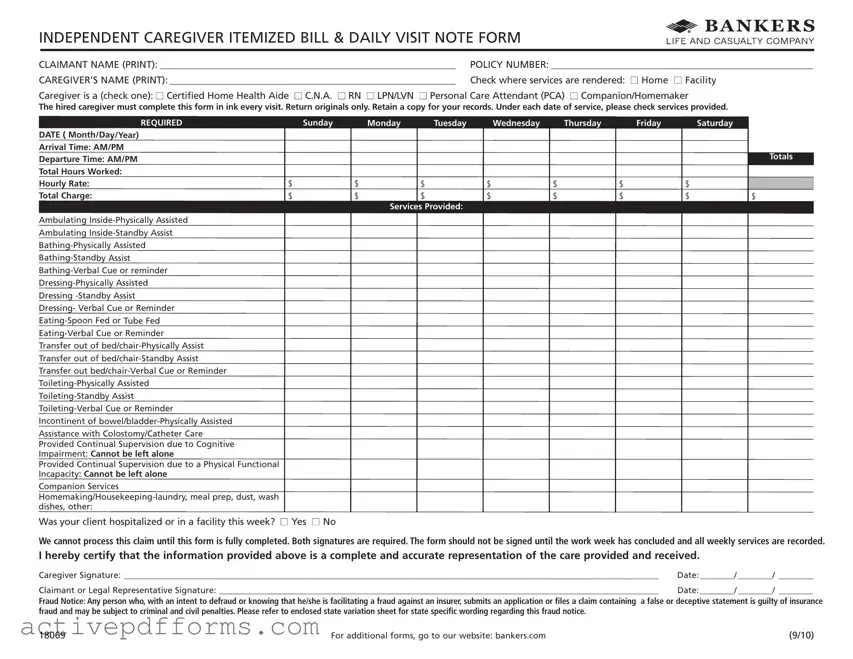
Managing the intricacies of caregiving responsibilities, especially for those working with individuals who require significant assistance, can be daunting without the right tools. One such indispensable tool is the Caregiver Daily Log form, designed to ensure that all aspects of care are meticulously documented and financial aspects are transparent for both the caregiver and the client. This form serves several critical functions: it acts as an itemized bill detailing the services rendered during each visit, a daily log of the caregiver's activities, and a record of the total hours worked along with the associated costs. Caregivers are prompted to check off specific services provided during their visit, ranging from assistance with mobility and personal care to meal preparation and housekeeping. Moreover, the form must be filled out in ink and requires the signatures of both the caregiver and the client or their legal representative at the end of each week, reinforcing accountability and providing a paper trail for both parties. This detailed documentation is crucial, not only for the calculation of charges but also for insurance purposes, as it includes a fraud notice highlighting the legal consequences of false claims. Utilizing this form ensures that caregiving transactions are conducted fairly and transparently, fostering trust between caregivers and those they serve.
INDEPENDENT CAREGIVER ITEMIZED BILL & DAILY VISIT NOTE FORM
CLAIMANT NAME (PRINT): _____________________________________________________________ |
POLICY NUMBER: ______________________________________________________ |
CAREGIVER’S NAME (PRINT): ___________________________________________________________ |
Check where services are rendered: n Home n Facility |
Caregiver is a (check one): n Certified Home Health Aide n C.N.A. n RN n LPN/LVN n Personal Care Attendant (PCA) n Companion/Homemaker
The hired caregiver must complete this form in ink every visit. Return originals only. Retain a copy for your records. Under each date of service, please check services provided.
REQUIRED
DATE ( Month/Day/Year)
Arrival Time: AM/PM
Departure Time: AM/PM
Total Hours Worked:
Hourly Rate:
Total Charge:
Sunday |
Monday |
Tuesday |
Wednesday |
Thursday |
Friday |
Saturday |
|
|
|
|
|
|
|
Totals |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
$ |
$ |
$ |
$ |
$ |
$ |
$ |
$ |
|
|
Services Provided: |
|
|
|
|
|
Ambulating
Assistance with Colostomy/Catheter Care Provided Continual Supervision due to Cognitive Impairment: Cannot be left alone Provided Continual Supervision due to a Physical Functional Incapacity: Cannot be left alone
Companion Services
meal prep, dust, wash |
Was your client hospitalized or in a facility this week? n Yes n No
We cannot process this claim until this form is fully completed. Both signatures are required. The form should not be signed until the work week has concluded and all weekly services are recorded.
I hereby certify that the information provided above is a complete and accurate representation of the care provided and received.
Caregiver Signature: ____________________________________________________________________________________________________________________________ |
Date: ________/ ________/ |
________ |
Claimant or Legal Representative Signature: ______________________________________________________________________________________________________ |
Date: ________/ ________/ |
________ |
Fraud Notice: Any person who, with an intent to defraud or knowing that he/she is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud and may be subject to criminal and civil penalties. Please refer to enclosed state variation sheet for state specific wording regarding this fraud notice.
18069 |
For additional forms, go to our website: bankers.com |
(9/10) |
| Fact Name | Description |
|---|---|
| Form Usage | This form is used by caregivers to itemize services provided during each visit, including hours worked and total charges. |
| Completion Requirement | The caregiver must complete this form in ink for every visit and retain a copy for their records. It cannot be processed unless fully completed and signed at the end of the work week. |
| Service Checklist | Services provided are detailed in a checklist format, covering a wide range of activities from physical assistance to companion services and housekeeping. |
| Governing Law | State-specific fraud notices apply, requiring reference to an enclosed variation sheet for precise wording. The form includes a fraud warning highlighting the criminal and civil penalties for submitting false or deceptive claims. |
Filling out the Caregiver Daily Log form is an important task that ensures accurate tracking and billing for caregiver services. This form serves as a detailed record of the care provided on a daily basis, capturing essential information such as the type of services rendered, hours worked, and charges incurred. To complete the form correctly and efficiently, it's helpful to follow a set of structured steps. This not only facilitates smooth processing but also helps in avoiding common errors.
Remember, the Caregiver Daily Log form is a legal document. Hence, ensuring the completeness and accuracy of every entry is paramount. Taking the time to double-check details can prevent misunderstandings and delays in processing. Once you have filled out the form, retain a copy for your records before submitting the original as instructed. This careful attention to detail will contribute to the smooth facilitation of care and support services.
What is the purpose of the Caregiver Daily Log form?
The Caregiver Daily Log form serves as a detailed record of the services provided by caregivers during their visits. It is designed to document the type of care given, including specific tasks performed, the arrival and departure times, total hours worked, and the total charges for the services. This form ensures that there is an accurate and complete representation of the care provided, which is essential for processing claims and for keeping personal records.
Who needs to fill out the Caregiver Daily Log form?
The caregiver who provides the services is responsible for filling out this form in ink for every visit. It’s important that the caregiver completes the form accurately, recording each service provided under the appropriate date, along with noting the start and end times of the visit, total hours worked, and the hourly rate charged.
What information is required on the form?
How often should the form be completed?
This form should be completed after each visit, ensuring every service provided is logged accurately. Caregivers must only submit the original completed forms, and they are encouraged to retain a copy for their records. The form should not be signed until all services for the work week have been documented and concluded.
Why is it important to fill out this form accurately?
Accurate completion of the form is crucial for several reasons: it enables caregivers to be fairly compensated for their services, ensures claimants can be reimbursed by insurance where applicable, and maintains a clear record for legal compliance. Inaccurate information could lead to delays in payment processing, disputes over services provided, and potential penalties for insurance fraud.
What happens if the form is not fully completed?
If any part of the form is left incomplete, the processing of the claim may be delayed or denied. Both the caregiver and the claimant/legal representative must ensure every section of the form is filled out correctly and that both signatures are provided at the end of the work week. This complete and signed form is then submitted for processing. Additionally, the inclusion of a fraud notice warns of the legal consequences of submitting false or deceptive statements.
When filling out a Caregiver Daily Log form, it's important to complete it accurately and attentively to ensure that the care provided is appropriately documented and reimbursed. However, people commonly make several mistakes that can complicate or delay this process. Knowing what these errors are can help caregivers avoid them. Here's an expanded list of mistakes often made:
Avoiding these mistakes can help ensure the form is filled out correctly, aiding in the smooth processing of care documentation and reimbursement. Always double-check your work and keep accurate records for each client to provide the best care possible.
When managing the care of an individual, whether due to aging, illness, or disability, a comprehensive approach is essential. Beyond the Caregiver Daily Log form, which provides a detailed record of the services provided during each visit, there are several other forms and documents that play vital roles in ensuring the health, safety, and well-being of the cared-for person.
Together, these documents form a comprehensive framework that supports the delivery of personalized, efficient, and effective care. Keeping these records accurate and up-to-date ensures that caregivers can provide the best possible assistance, while also meeting legal and healthcare requirements. Whether used in a professional setting or within the home, these tools are essential for anyone responsible for the care of an individual.
Medical Appointment Summary: Similar to the Caregiver Daily Log form, Medical Appointment Summaries often include detailed information about the patient's visit, including the date and time, the type of healthcare professional seen, and the services provided. Both documents serve as a record of the interaction and care given during a specific period.
Home Health Aide Timesheet: This document, like the Caregiver Daily Log form, tracks the hours worked by a caregiver in a home or facility setting. It typically includes arrival and departure times, total hours worked, and sometimes the specific tasks performed during the visit. Both forms are essential for payroll and billing purposes, ensuring accurate compensation for services rendered.
Patient Care Report (PCR): Commonly used in emergency medical services, the PCR provides a detailed account of the medical care and support provided to a patient during an emergency call-out. While its context might differ, its function mirrors the Caregiver Daily Log in documenting key services provided, patient responses, and the professional's observations. Both are crucial for continuity of care and insurance purposes.
Personal Care Plan: This document outlines the specific care needs and services to be provided to an individual, often within a home care setting. Similar to the Caregiver Daily Log form, it includes detailed instructions for daily activities, support levels required (e.g., physical assistance, verbal cues), and any specialized care needs. While the Care Plan is more of a guideline, and the Daily Log is a record, both work together to ensure the patient's needs are met comprehensively.
When you're filling out the Caregiver Daily Log form, it's important to make sure every entry is clear and accurate. To help you navigate this process, here's a list of dos and don'ts that you should consider:
Do:Following these guidelines can help ensure that the Caregiver Daily Log form is completed thoroughly and accurately, facilitating a smoother process for both the caregiver and the claimant.
When it comes to caregiving, accurate documentation is crucial, not only for ensuring the delivery of quality care but also for legal and financial accountability. The "Caregiver Daily Log Form" is a tool designed to assist in this documentation process. However, misconceptions surrounding its use and importance often lead to its underutilization or misuse. Here are eight common misconceptions about the Caregiver Daily Log form:
Addressing these misconceptions is essential for caregivers, claimants, and legal representatives alike. By fostering a better understanding of the Caregiver Daily Log form's purpose and requirements, all parties can ensure that the caregiving process is accurately documented, promoting transparency and accountability in caregiver-client relationships.
When filling out and using the Caregiver Daily Log form, there are several key takeaways to ensure accurate and effective recording of services provided. These not only help in managing the logistics of caregiving but also ensure that all parties are appropriately informed and compliant with necessary regulations.
Utilizing the Caregiver Daily Log form with diligence and attention to detail ensures transparency, accountability, and compliance in the caregiving environment. It serves as a vital piece of documentation for all parties involved, facilitating not only billing and legal processes but also encouraging best practices in home health care.
Poker Run Rules - Mandating separate tally sheets for playing multiple hands ensures that each hand is accounted for accurately and fairly.
What Is a Tax Receipt for Donations - Two bags of baby clothes and accessories, gently used.
Printable:jdpfykbvz18= Yahtzee Score Card - Supports strategic decision-making by letting players easily assess which scoring categories are best to pursue.