Free Cms 485 PDF Template
Free Cms 485 PDF Template
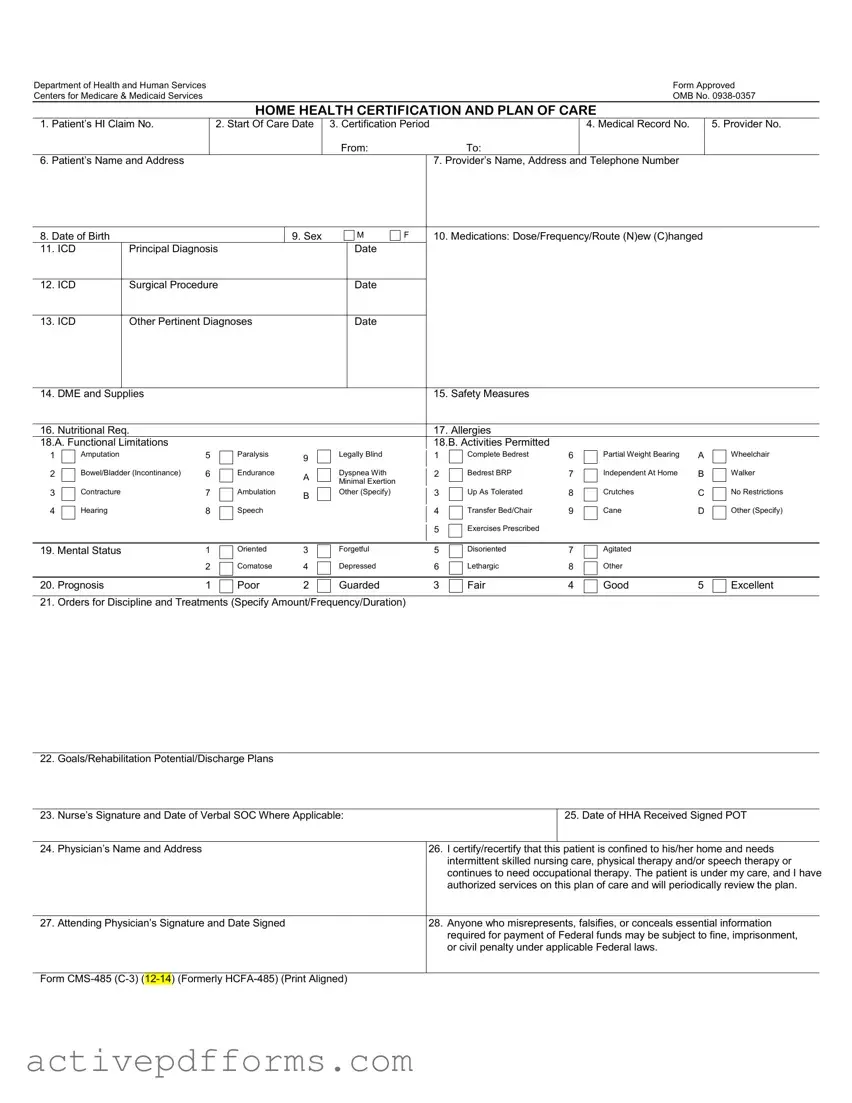
Navigating healthcare administration can often seem like a complex labyrinth, especially when it comes to ensuring that patients receive the care they need while complying with federal guidelines. At the heart of this process for home health services lies the CMS-485 form, a crucial document drafted by the Department of Health and Human Services and approved by the Centers for Medicare & Medicaid Services. This form, known formally as the Home Health Certification and Plan of Care, serves a multifaceted purpose, including certifying that a patient is homebound and detailing the home healthcare services they require. It encompasses a vast array of information critical to patient care, from personal identification and medical history, including diagnoses and medications, to the specific healthcare services and equipment needed. Additionally, the form outlines safety measures, nutritional requirements, functional limitations, and the mental status of the patient, while setting forth the prognosis, treatment orders, goals, and plans for rehabilitation or discharge. Moreover, it demands the endorsement of the attending physician, affirming that the patient requires and is under the direct care for the services outlined, thereby playing a pivotal role in the authorization and continuation of home health services. Compliance and accuracy in filling out this form are not only necessary for the well-being of the patient but also play a critical role in the processing and payment of Medicare benefits, underlining its importance in the interface between clinical care and administrative support.
Department of Health and Human Services |
Form Approved |
Centers for Medicare & Medicaid Services |
OMB No. |
HOME HEALTH CERTIFICATION AND PLAN OF CARE
1. |
Patient’s HI Claim No. |
2. Start Of Care Date |
3. Certification Period |
|
4. Medical Record No. |
5. Provider No. |
|
|
|
From: |
To: |
|
|
6. |
Patient’s Name and Address |
|
|
7. Provider’s Name, Address and Telephone Number |
|
|
8. Date of Birth |
|
9. Sex |
M |
F |
10. Medications: Dose/Frequency/Route (N)ew (C)hanged |
11. ICD |
Principal Diagnosis |
|
Date |
|
|
|
|
|
|
|
|
12. ICD |
Surgical Procedure |
|
Date |
|
|
|
|
|
|
|
|
13. ICD |
Other Pertinent Diagnoses |
|
Date |
|
|
|
|
|
|
|
|
14. |
DME and Supplies |
15. |
Safety Measures |
|
|
|
|
16. |
Nutritional Req. |
17. |
Allergies |
18.A. Functional Limitations |
18.B. Activities Permitted |
||
1
2
3
4
Amputation |
5 |
|
Paralysis |
9 |
|
|
|
|
|
Bowel/Bladder (Incontinance) |
6 |
|
Endurance |
A |
|
||||
|
|
|
|
|
Contracture |
7 |
|
Ambulation |
B |
|
||||
|
|
|
|
|
Hearing |
8 |
|
Speech |
|
|
|
|||
|
|
|
|
|
Legally Blind
Dyspnea With
Minimal Exertion
Other (Specify)
1
2
3
4
5
Complete Bedrest |
6 |
Bedrest BRP |
7 |
Up As Tolerated |
8 |
Transfer Bed/Chair |
9 |
Exercises Prescribed |
|
Partial Weight Bearing |
A |
Independent At Home |
B |
Crutches |
C |
Cane |
D |
Wheelchair
Walker
No Restrictions
Other (Specify)
19. Mental Status |
1 |
Oriented |
3 |
Forgetful |
5 |
Disoriented |
7 |
Agitated |
|
|
|
2 |
Comatose |
4 |
Depressed |
6 |
Lethargic |
8 |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Prognosis |
1 |
Poor |
2 |
Guarded |
3 |
Fair |
4 |
Good |
5 |
Excellent |
21. Orders for Discipline and Treatments (Specify Amount/Frequency/Duration)
22. Goals/Rehabilitation Potential/Discharge Plans
23. Nurse’s Signature and Date of Verbal SOC Where Applicable:
25. Date of HHA Received Signed POT
24. |
Physician’s Name and Address |
26. |
I certify/recertify that this patient is confined to his/her home and needs |
|
|
|
|
intermittent skilled nursing care, physical therapy and/or speech therapy or |
|
|
|
|
continues to need occupational therapy. The patient is under my care, and I have |
|
|
|
|
authorized services on this plan of care and will periodically review the plan. |
|
|
|
|
|
|
27. |
Attending Physician’s Signature and Date Signed |
28. |
Anyone who misrepresents, falsifies, or conceals essential information |
|
|
|
|
required for payment of Federal funds may be subject to fine, imprisonment, |
|
|
|
|
or civil penalty under applicable Federal laws. |
|
|
|
|
|
|
Form
Privacy Act Statement
Sections 1812, 1814, 1815, 1816, 1861 and 1862 of the Social Security Act authorize collection of this information. The primary use of this information is to process and pay Medicare benefits to or on behalf of eligible individuals. Disclosure of this information may be made to: Peer Review Organizations and Quality Review Organizations in connection with their review of claims, or in connection with studies or other review activities, conducted pursuant to Part B of Title XI of the Social Security Act; State Licensing Boards for review of unethical practices or nonprofessional conduct; A congressional office from the record of an individual in response to an inquiry from the congressional office at the request of that individual.
Where the individual’s identification number is his/her Social Security Number (SSN), collection of this information is authorized by Executive Order 9397. Furnishing the information on this form, including the SSN, is voluntary, but failure to do so may result in disapproval of the request for payment of Medicare benefits.
Paper Work Burden Statement
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
| Fact Name | Description |
|---|---|
| Form Designation | CMS-485, HOME HEALTH CERTIFICATION AND PLAN OF CARE |
| Approval Authority | Department of Health and Human Services, Centers for Medicare & Medicaid Services |
| OMB Control Number | 0938-0357 |
| Form Purpose | The form is used to certify that a patient is homebound and requires home health services, outlining the plan of care. |
| Key Sections | Includes patient information, certification period, medical diagnosis, medications, functional limitations, treatments, and physician certification. |
| Legal Base | Sections 1812, 1814, 1815, 1816, 1861, and 1862 of the Social Security Act |
| Paperwork Reduction Act Statement | Displays valid OMB control number 0938-0357 with an estimated completion time of 15 minutes per response. |
| Penalty for False Statements | Subjects to fine, imprisonment, or civil penalty under applicable Federal laws for misrepresentation, falsification, or concealment of essential information. |
Filling out the CMS 485 form, officially known as the Home Health Certification and Plan of Care, is a critical step in securing Medicare benefits for home health services. This document is essentially a blueprint for the patient's home health care, detailing the services approved by a physician. Accuracy and clarity in completing this form are paramount, as it guides the delivery of care and ensures compliance with Medicare requirements. Here is a step-by-step guide to help you navigate through the completion process smoothly.
Upon completion, the CMS 485 form acts as a vital communication tool among health care providers, ensuring everyone involved in the patient's care is informed of the plan and their respective roles. Thoroughly review the entire form before submission to avoid delays in care or payment. With this guide, the task of completing the CMS 485 form should be more straightforward, setting a clear path for the necessary home health services the patient requires.
What is the CMS-485 form?
The CMS-485 form is a document approved by the Department of Health and Human Services and the Centers for Medicare & Medicaid Services. It serves as a Home Health Certification and Plan of Care, outlining the necessary information needed for a patient's home health services, including patient identification, medical and treatment plans, medications, and provider details.
Who needs to complete the CMS-485 form?
This form must be completed by a patient's attending physician or a qualified healthcare provider who is overseeing the patient's home health care. It should be filled out in collaboration with the home health agency providing the services.
What information is required on the CMS-485 form?
The form requires detailed information about the patient, including their Medicare claim number, start of care date, medical record number, name, address, and other personal information. Additionally, it requires a comprehensive treatment plan consisting of medications, diagnoses, medical equipment, safety measures, and specific orders for discipline and treatments alongside the goals and potential rehabilitation plans.
How is the CMS-485 form used?
The primary use of this form is to document and communicate a patient's home health care plan involving skilled nursing care, physical, speech, and/or occupational therapy. It serves as a formal certification of the necessity for home health services under Medicare guidelines and is used to authorize and process Medicare payments for these services.
Is the CMS-485 form mandatory for receiving home health services under Medicare?
Yes, for Medicare beneficiaries requiring home health services, the completion and submission of a CMS-485 form is necessary. It certifies the patient's eligibility for home health care and is a requirement for the Medicare payment process.
Can the CMS-485 form be revised after it's submitted?
Yes, the CMS-485 form can be updated or revised as the patient's condition changes or if there is a need to modify the care plan. Such revisions must be signed off by the attending physician or authorized healthcare provider to remain effective and compliant.
What is the validity period of a CMS-485 form?
The form outlines a certification period for the plan of care, which typically aligns with the 60-day benefit period under Medicare's home health benefit. The care plan can be recertified for subsequent periods as medically necessary.
How is patient privacy protected with the CMS-485 form?
Protection of patient information is mandated under the Privacy Act Statement included in the form. The information collected is primarily used for processing Medicare benefits, with limited, authorized disclosure under specific, regulated circumstances to ensure patient privacy and confidentiality.
What are the consequences of failing to complete the CMS-485 form accurately?
Inaccuracies or failure to provide the required information on the CMS-485 form can result in disapproval of payment for Medicare benefits. Additionally, the form note specifies potential legal consequences, including fines, imprisonment, or civil penalty for misrepresentation or falsification of essential information.
Where can I find more information or assistance with the CMS-485 form?
Additional guidance and assistance with the CMS-485 form can be obtained from the Centers for Medicare & Medicaid Services (CMS) directly or through a healthcare provider experienced in home health services. The CMS website and your local Medicare office are valuable resources for questions and support.
Filling out the CMS-485 form, also known as the Home Health Certification and Plan of Care, is a crucial step for healthcare providers to ensure that patients receive the Medicare benefits they're entitled to for home health services. Despite its importance, errors frequently occur during the completion process. Here are seven common mistakes:
Ensuring the CMS-485 form is filled out accurately and completely is paramount for healthcare providers. This not only facilitates proper care but also ensures compliance with Medicare's regulations. Giving attention to detail, double-checking for accuracy, and understanding the purpose of each section can mitigate these common errors, leading to smoother processing and better patient outcomes.
The CMS-485 form, also known as the Home Health Certification and Plan of Care, is a critical document within the realm of home healthcare, facilitating the process of obtaining Medicare benefits for eligible individuals who require home-based care. This form, approved by the Department of Health and Human Services and the Centers for Medicare & Medicaid Services, serves as a comprehensive plan covering a vast array of patient information, including medical diagnosis, prescribed medications, and the specific care needed. While it stands as a cornerstone document, several other forms and documents often accompany the CMS-485 to ensure thorough patient care and compliance with healthcare regulations.
Together with the CMS-485 form, these documents form a robust framework to support the delivery of high-quality home health care services. By integrating patient-specific data, regulatory requirements, and safety protocols, healthcare professionals are better equipped to tailor care plans that address individual needs while ensuring that the necessary legal and procedural standards are met. This holistic approach underlines the importance of comprehensive documentation in facilitating effective care and achieving optimal health outcomes for patients receiving home health services.
The Skilled Nursing Facility Advanced Beneficiary Notice (SNFABN, Form CMS-10055) is similar to the CMS-485 form because both pertain to the care planning and notification processes required for Medicare beneficiaries. While the CMS-485 is a certification and plan of care for home health patients, the SNFABN informs SNF patients about items and services Medicare may not cover.
Outcome and Assessment Information Set (OASIS) is another document related to the CMS-485 form, focusing on home health care. OASIS is used for gathering patient data that informs care planning, similar to how the CMS-485 form outlines a plan of care but is specifically designed for assessing outcomes in home health scenarios.
The Physician Order for Life-Sustaining Treatment (POLST) form shares similarities with the CMS-485 in that both involve directives concerning a patient's care. However, the POLST is more specifically aimed at indicating a patient's preferences regarding life-sustaining treatments across all healthcare settings, not just home health care.
A Medication Administration Record (MAR) can be parallel to the medication details section found in the CMS-485 form. Both documents track the medications a patient is taking, including dosage and frequency, which is essential for ensuring proper medical care in home health environments.
The Home Health Advance Beneficiary Notice (HHABN, Form CMS-R-296) is quite similar to the CMS-485. The HHABN informs beneficiaries about services and items that Medicare may not cover, while the CMS-485 specifies the plan of care, including covered services. Both are integral to the communication process between care providers and patients in home health services.
Individualized Plan of Care (IPC) in other healthcare settings, like hospice or long-term care, resembles the CMS-485 as both forms document the care plan tailored to a patient's specific needs. The IPC is broader in application but serves a similar purpose in ensuring that a patient’s health needs are identified and met according to a structured plan.
Filling out the CMS-485 form, also known as the Home Health Certification and Plan of Care, is a critical process for healthcare providers. It helps to ensure that patients receive the appropriate home health care services covered under Medicare. As such, it's crucial to complete this form accurately and thoroughly. Below is a comprehensive guide on what to do and what not to do when filling out this form.
By adhering to these guidelines, healthcare providers can help ensure the CMS-485 form is accurately completed, ultimately facilitating better care coordination and delivery for patients receiving home health services.
There are several misconceptions about the CMS-485 form, officially known as the Home Health Certification and Plan of Care. Understanding what the form is and its use is critical for healthcare professionals, patients, and caregivers involved in home health care under Medicare. Here are eight common misconceptions:
This is incorrect. The CMS-485 form is a mandatory document for Medicare to cover home health services. It serves as both a certification of patient eligibility and a detailed plan of care.
Actually, while various healthcare professionals can contribute to the plan of care, the attending physician must certify that home health services are necessary and sign off on the form for it to be valid.
Contrary to this belief, the CMS-485 must be updated and recertified at the beginning of each certification period to continue home health services under Medicare, reflecting any changes in the patient's condition or care plan.
While physicians play a critical role in authorizing the form, it actually requires a team approach. Home health agencies, nurses, and other care providers use the form to understand the patient's care plan, making it a vital communication tool.
This form encompasses a broad range of care needs, including medical treatments, safety measures, nutritional requirements, and any durable medical equipment and supplies.
The reality is that electronic submission of CMS-485 is permitted and even encouraged as it can expedite the approval process and ensure the seamless continuation of care.
In fact, amendments to the CMS-485 are common and necessary when a patient's condition or care needs change. The attending physician must approve these revisions.
Quite the contrary, the form is subject to privacy regulations under the Health Insurance Portability and Accountability Act (HIPAA), ensuring confidential handling of patient information.
Clarifying these misconceptions is crucial for the accurate and effective use of the CMS-485 form in the provision of home health services. This form not only facilitates proper care planning and reimbursement but also ensures compliance with federal regulations governing Medicare-covered home health services.
Filling out the CMS 485 form is crucial for ensuring proper care and support for patients under home health services through Medicare. Here are nine key takeaways regarding the completion and utilization of this form:
Comprehensive and accurate completion of the CMS 485 form is fundamental in facilitating effective care coordination and management for patients receiving home health services. It serves as a critical document in aligning healthcare providers, services, and patient needs under the Medicare program.
Philadelphia Electric Company - Guidance on PECO service requests for commercial properties, including service relocation or upgrade.
Itemized Fee Worksheet - Helps navigate the financial aspects of buying a home by breaking down complex fees into understandable parts.