Free Cna Shower Sheets PDF Template
Free Cna Shower Sheets PDF Template
The CNA Shower Sheets form is a critical tool designed to ensure comprehensive skin monitoring for residents in care facilities, particularly during routine showers. This form serves a dual purpose: firstly, it guides certified nursing assistants (CNAs) to perform a thorough visual assessment of a resident's skin, and secondly, it ensures any abnormalities are promptly reported. Important aspects covered by the form include the identification and description of a wide range of skin issues, such as bruising, rashes, swelling, dryness, lesions, and changes in skin temperature or color, among others. By recording the exact location and nature of these abnormalities using a detailed body chart, the form facilitates accurate communication between CNAs, charge nurses, and, if necessary, the Director of Nursing (DON). It is a crucial document for initiating swift intervention and ensuring the well-being of residents. Moreover, this form, prepared by Primaris and adapted from Ratlif Care Center, underscores the importance of meticulous skin care in preventing complications and fostering overall resident health, while also aligning with standards set forth by the Centers for Medicare & Medicaid Services (CMS).
Skin Monitoring: Comprehensive CNA Shower Review
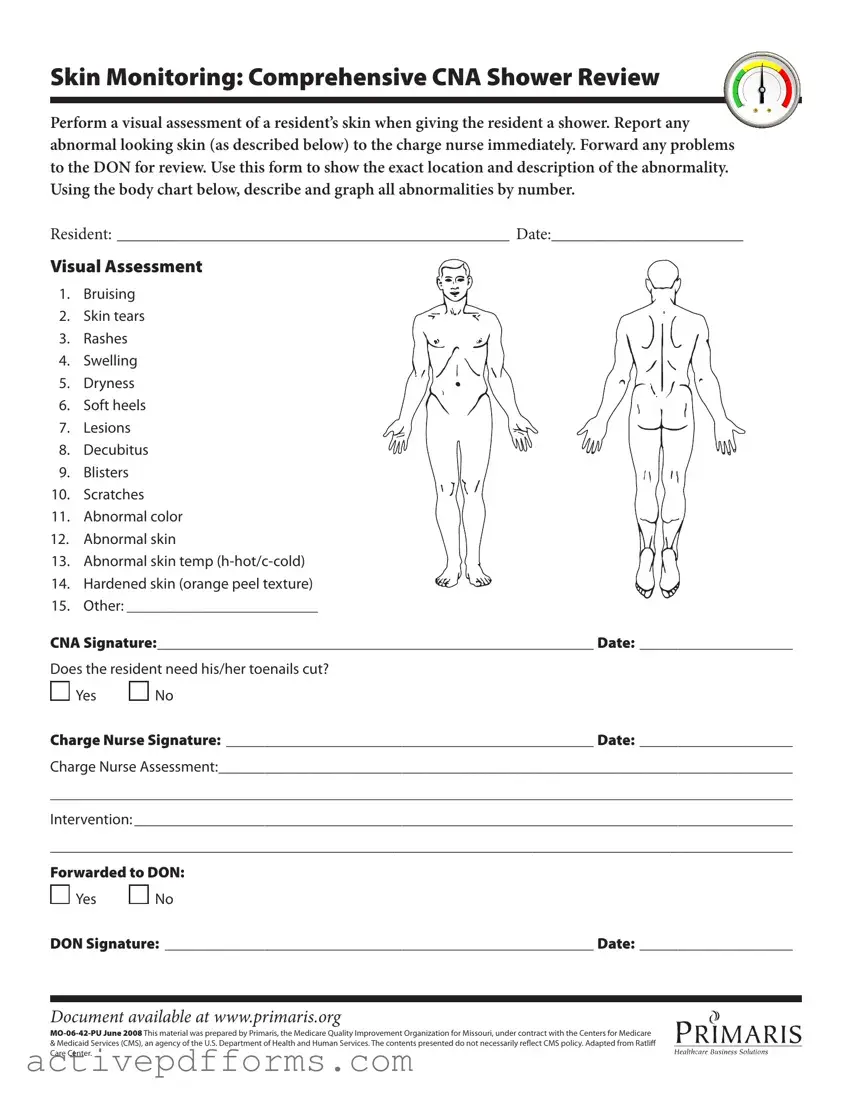
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
| Fact | Description |
|---|---|
| Purpose of Form | Used for performing a visual assessment of a resident's skin during a shower and documenting any abnormalities. |
| Abnormalities to Report | Bruising, skin tears, rashes, swelling, dryness, soft heels, lesions, decubitus, blisters, scratches, abnormal color, abnormal skin, temperature variations, hardened skin, among others. |
| Reporting Process | Any observed abnormalities should be reported immediately to the charge nurse and forwarded to the Director of Nursing (DON) for review. |
| Body Chart Usage | The form includes a body chart to describe and graphically represent the location and description of the skin abnormalities. |
| Additional Assessments | Question regarding the need for toenail cutting is included, highlighting the comprehensive nature of the assessment. |
| Signature Requirements | Signatures from the CNA, charge nurse, and DON are required, indicating a multi-level review process. |
| Document Source | The form is available on Primaris' website and is developed for the state of Missouri. |
| Governing Law(s) | Governed under Missouri State Law and adapted from Ratliff Care Center's guidelines, with oversight from CMS and HHS. |
| Preparation and Approval | Prepared by Primaris, the Medicare Quality Improvement Organization for Missouri, under contract with the CMS. |
| Adaptation | Adapted from procedures used at Ratlif Care Center, suggesting collaboration and best practice sharing within the care community. |
Completing the CNA Shower Sheets form is a meticulous process that requires attention to detail to ensure accurate and comprehensive documentation of any abnormalities found on a resident’s skin during showering. This documentation is crucial as it facilitates timely intervention by the nursing team and ensures that resident care is managed effectively. Following the outlined steps will assist in filling out the form properly.
Once the form is fully completed and signed by the necessary parties, it becomes a part of the resident's medical record. This record assists in ongoing care planning and must be handled with confidentiality and professionalism. The thorough documentation process ensures that all team members are informed of the resident's condition and can provide appropriate care as needed.
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to document and track any abnormalities observed on a resident's skin during a shower. It provides a structured way for a Certified Nursing Assistant (CNA) to perform a visual assessment and record findings such as bruises, rashes, swelling, and other conditions. The form facilitates immediate reporting to the charge nurse and subsequent review by the Director of Nursing (DON). This process ensures prompt attention to any potential health issues.
How should a CNA use this form?
A CNA should use this form every time they give a resident a shower. During the shower, the CNA performs a visual assessment of the resident's skin, looking for any signs listed on the form. If any abnormalities are found, the CNA records the exact location and description on the form, using the body chart provided. The CNA then signs and dates the form and reports the findings to the charge nurse immediately for further assessment and intervention.
What should be done if an abnormality is found?
If an abnormality is noted on a resident's skin, the CNA must immediately report this to the charge nurse. The detailed description and location of the abnormality should be clearly documented on the form. The charge nurse will then assess the situation, decide on the necessary intervention, and may forward the information to the Director of Nursing (DON) for further review and action. Prompt reporting and documentation are crucial for the resident's timely care and health monitoring.
Are there specific abnormalities that should be reported?
Yes, the form lists specific types of skin abnormalities that should be reported. These include bruising, skin tears, rashes, swelling, dryness, soft heels, lesions, decubitus (bedsores), blisters, scratches, abnormal color, abnormal skin texture, abnormal skin temperature (hot or cold), hardened skin (with an orange peel texture), and other conditions not specifically listed. Any condition out of the ordinary should be documented and reported.
What happens after the form is forwarded to the DON?
After the form is forwarded to the Director of Nursing (DON), they review the documented skin abnormalities, assess the resident's needs, and may initiate further medical examination or treatment. The DON is also responsible for overseeing the implementation of any recommended interventions and for ensuring that appropriate follow-up care is provided. This step is crucial for managing resident health conditions effectively and preventing complications.
Is it mandatory to report normal findings?
While the form is primarily intended for documenting and reporting abnormalities, it is also vital to complete the form even if no abnormalities are found during the visual assessment. This practice ensures a consistent review process is followed for every shower given to a resident, providing a complete and accurate record of the resident's skin condition over time. Regular documentation, even of normal findings, helps in monitoring the resident's health and well-being efficiently.
Common mistakes when filling out the CNA Shower Sheets form are varied and can significantly impact the care process if not addressed properly. These errors can hinder effective communication among healthcare team members and compromise patient care quality. It's crucial to pay close attention to detail when completing this form to ensure accurate and comprehensive documentation of skin assessments.
To ensure the form is filled out correctly and thoroughly, healthcare providers should:
By avoiding these common mistakes and following the corrective steps, healthcare providers can ensure a more efficient and effective skin monitoring process, ultimately contributing to better resident care.
When professionals in the healthcare sector employ the CNA Shower Sheets form, they are engaging with just one part of a comprehensive documentation system designed to assure the well-being, safety, and proper care of residents in long-term care facilities. The CNA Shower Sheets form plays a pivotal role in mapping out a visual assessment of a resident’s skin conditions during shower routines, enabling timely identification and response to any irregularities. However, to maintain a holistic view and support effective care planning, this form is often used in concert with several other documents, each contributing its unique value to the overall care process.
The use of the CNA Shower Sheets form alongside these additional documents creates a multidimensional approach to resident care, enabling a seamless integration of insights that foster well-rounded care regimes. By capturing detailed information across various aspects of care, healthcare providers can optimize their care strategies, making informed decisions that elevate the quality of life for residents. Together, these forms and documents encapsulate a commitment to diligent, compassionate care, in which every action and intervention is guided by a deep understanding of the individual needs of each resident.
**Wound Assessment Forms**: Similar to the CNA Shower Sheets form, these documents are used in healthcare settings, particularly in nursing or care homes, to document the condition of a patient's wounds. Both types of forms focus on visual assessments, noting features such as size, location, color, and type of wound or skin abnormality. The goal is to track changes over time and ensure timely medical intervention.
**Patient Admission Assessment Forms**: These documents are used when a patient is admitted to a healthcare facility and include comprehensive evaluations of the patient’s physical and health status. Like the CNA Shower Sheets form, they require detailed documentation of any existing conditions, including skin issues, to provide a baseline for future care and to identify any immediate needs for intervention.
**Medication Administration Records (MAR)**: While MARs primarily track the administration of medications to individuals in healthcare settings, they share a common emphasis on accuracy, detail, and timeliness with CNA Shower Sheets. Both forms contribute to the continuum of care, ensuring that all staff are informed of the patient's current condition and any treatments provided.
**Daily Nursing Notes**: These notes are a continuous record of a patient's day-to-day condition, treatments received, and any changes in their well-being. Like the CNA Shower Sheets, Daily Nursing Notes serve as a communication tool among healthcare providers, offering insights into the patient's health status and any observed changes, including those related to skin integrity and abnormalities.
**Incident Reports**: Used to document any unusual or unexpected events affecting patient care, Incident Reports share similarities with CNA Shower Sheets in their focus on specifics, such as the detailed description of the incident (or in the case of the CNA form, the skin abnormality), actions taken, and outcomes. Both are critical for legal compliance, quality assurance, and improving patient care practices.
When filling out the CNA Shower Sheets form, certain practices should be followed to ensure the accuracy and completeness of the documentation. Below are guidelines that highlight what should and shouldn't be done during this process.
Following these dos and don'ts will ensure the CNA Shower Sheets form is filled out comprehensively and accurately, reinforcing the high standard of care provided to residents.
When it comes to the CNA Shower Sheets form, there are several misconceptions that can lead to its improper use or misinterpretation. Below are seven common myths and the truths behind them:
Careful and accurate use of the CNA Shower Sheets form is essential in monitoring and maintaining the skin health of residents, thereby preventing potential health issues and ensuring high-quality care.
Understanding how to properly utilize the CNA Shower Sheets form plays a crucial role in ensuring the wellness and care of residents in healthcare facilities. Here are some key takeaways for healthcare professionals.
The primary goal of the CNA Shower Sheets form is to serve as a tool for the visual assessment of a resident’s skin during shower times. This process is pivotal in identifying any skin abnormalities early on.
It is imperative to report any abnormal skin findings, such as bruising, rashes, swelling, dryness, or any other listed conditions, to the charge nurse immediately. Prompt reporting can significantly impact the resident's health by facilitating early intervention.
The form requires detailed documentation, including the exact location and description of the skin abnormality. This information is crucial for ensuring that the healthcare team can accurately monitor and treat any conditions without delay.
The role of the CNA (Certified Nursing Assistant) in this process is both proactive and reactive. While they are responsible for the initial identification and documentation of skin concerns, their observations must be forwarded to the Director of Nursing (DON) for further review, indicating a collaborative approach to resident care.
Accurate and timely documentation on the CNA Shower Sheets form not only fosters effective communication among the healthcare team but also plays a vital role in the ongoing health and well-being of the residents under their care. It underlines the importance of attention to detail and the necessity for all staff to be vigilant and proactive in their roles.
Employee Disciplinary Action Form - Facilitates a structured disciplinary process, allowing for an accurate record of employee infractions and the actions taken by management.
Chain Of Custody - A detailed chronology of a signet ring implicated in a fraud case, from its initial discovery to verification of historical significance and forensic comparison with documents.