Free Db 450 Disability PDF Template
Free Db 450 Disability PDF Template
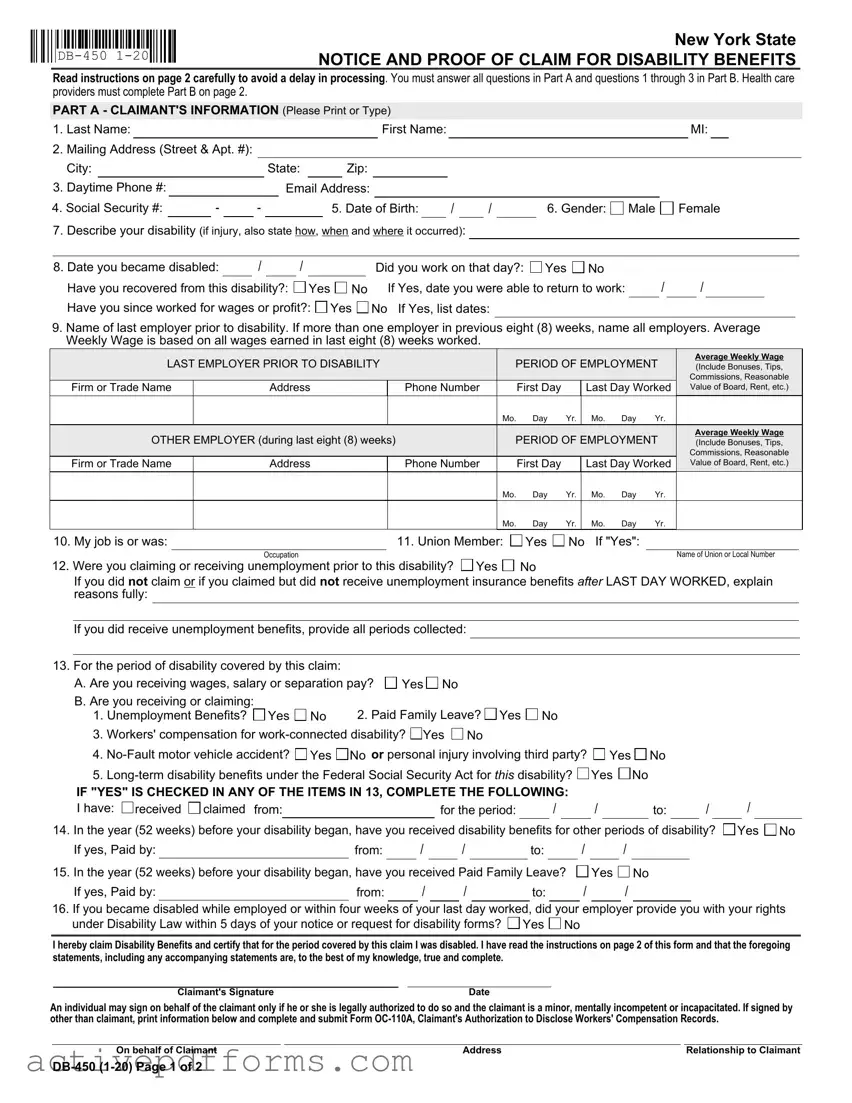
The DB-450 form is a critical document for New Yorkers navigating the complexities of claiming disability benefits. Officially recognized as the "Notice and Proof of Claim for Disability Benefits," this form is your gateway to ensuring that you receive the support you're entitled to during a challenging period. Structured in two main parts, the form first gathers comprehensive information about the claimant, including personal identification, employment details, the nature of the disability, and any prior claims for benefits. Notably, it requires clear documentation regarding the onset date of the disability and any wages earned in the period leading up to it. Moreover, to strengthen the claim, Part B demands a detailed medical assessment from a healthcare provider, ensuring that all details regarding the diagnosis, treatment, and projected recovery are thoroughly documented. To prevent processing delays, the form emphasizes the importance of answering every question meticulously. Commanding attention in this process is the stipulation for timely submission, guided by whether the disability occurred during employment or after a period of unemployment. The instructions also touch upon the interplay with other benefits such as unemployment benefits, workers' compensation, and even no-fault motor vehicle incidents, amongst others. Ensuring accuracy and completeness when filling out this form not only expedites the claim process but also supports New Yorkers in their time of need, reinforcing the safety nets that the state has in place for its residents facing temporary disabilities.
New York State |
|
NOTICE AND PROOF OF CLAIM FOR DISABILITY BENEFITS |
Read instructions on page 2 carefully to avoid a delay in processing. You must answer all questions in Part A and questions 1 through 3 in Part B. Health care providers must complete Part B on page 2.
PART A - CLAIMANT'S INFORMATION (Please Print or Type)
1. |
Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name: |
|
|
|
|
|
|
|
MI: |
|
|
|||
2. |
Mailing Address (Street & Apt. #): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
City: |
|
|
|
|
|
|
State: |
|
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Daytime Phone #: |
|
|
|
|
|
|
Email Address: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
4. Social Security #: |
|
- |
|
- |
|
|
|
5. Date of Birth: |
|
|
/ |
|
/ |
|
6. Gender: |
Male |
Female |
|
||||||||||
7.Describe your disability (if injury, also state how, when and where it occurred):
8. Date you became disabled: |
|
/ |
|
/ |
|
|
|
Did you work on that day?: Yes No |
/ |
/ |
|
|
||
Have you recovered from this disability?: |
|
Yes |
No |
If Yes, date you were able to return to work: |
|
|
||||||||
Have you since worked for wages or profit?: |
Yes |
No If Yes, list dates: |
|
|
|
|
|
|
||||||
9.Name of last employer prior to disability. If more than one employer in previous eight (8) weeks, name all employers. Average Weekly Wage is based on all wages earned in last eight (8) weeks worked.
LAST EMPLOYER PRIOR TO DISABILITY |
|
PERIOD OF EMPLOYMENT |
Average Weekly Wage |
|||||||
|
(Include Bonuses, Tips, |
|||||||||
|
|
|
|
|
|
|
|
|
|
Commissions, Reasonable |
Firm or Trade Name |
Address |
|
Phone Number |
|
First Day |
|
Last Day Worked |
Value of Board, Rent, etc.) |
||
|
|
|
|
Mo. |
Day |
Yr. |
Mo. |
Day |
Yr. |
|
OTHER EMPLOYER (during last eight (8) weeks) |
|
PERIOD OF EMPLOYMENT |
Average Weekly Wage |
|||||||
|
(Include Bonuses, Tips, |
|||||||||
|
|
|
|
|
|
|
|
|
|
Commissions, Reasonable |
Firm or Trade Name |
Address |
|
Phone Number |
|
First Day |
|
Last Day Worked |
Value of Board, Rent, etc.) |
||
|
|
|
|
Mo. |
Day |
Yr. |
Mo. |
Day |
Yr. |
|
|
|
|
|
Mo. |
Day |
Yr. |
Mo. |
Day |
Yr. |
|
10. My job is or was: |
|
11. Union Member: |
Yes |
No If "Yes": |
||
|
Occupation |
|
|
|
|
Name of Union or Local Number |
12. Were you claiming or receiving unemployment prior to this disability? |
Yes |
No |
|
|
||
If you did not claim or if you claimed but did not receive unemployment insurance benefits after LAST DAY WORKED, explain reasons fully:
If you did receive unemployment benefits, provide all periods collected:
13. For the period of disability covered by this claim: |
|
|
|
A. Are you receiving wages, salary or separation pay? |
Yes No |
||
B. Are you receiving or claiming: |
|
2. Paid Family Leave? Yes No |
|
1. Unemployment Benefits? |
Yes No |
||
3.Workers' compensation for  Yes
Yes  No
No
4. Yes
Yes  No or personal injury involving third party?
No or personal injury involving third party?  Yes
Yes  No
No
5. Yes
Yes  No
No
IF "YES" IS CHECKED IN ANY OF THE ITEMS IN 13, COMPLETE THE FOLLOWING:
I have: |
received |
claimed from: |
|
for the period: |
|
/ |
|
/ |
|
to: |
|
/ |
14. In the year (52 weeks) before your disability began, have you received disability benefits for other periods of disability?
If yes, Paid by: |
|
from: |
|
/ |
|
/ |
|
to: |
|
/ |
|
/ |
/

 Yes
Yes 
 No
No
15. In the year (52 weeks) before your disability began, have you received Paid Family Leave?
If yes, Paid by: |
from: |
/ |
/ |
to: |
Yes
/
No
/
16.If you became disabled while employed or within four weeks of your last day worked, did your employer provide you with your rights under Disability Law within 5 days of your notice or request for disability forms?  Yes
Yes  No
No
I hereby claim Disability Benefits and certify that for the period covered by this claim I was disabled. I have read the instructions on page 2 of this form and that the foregoing statements, including any accompanying statements are, to the best of my knowledge, true and complete.
Claimant's Signature |
Date |
An individual may sign on behalf of the claimant only if he or she is legally authorized to do so and the claimant is a minor, mentally incompetent or incapacitated. If signed by other than claimant, print information below and complete and submit Form
On behalf of Claimant |
Address |
Relationship to Claimant |
PART B - HEALTH CARE PROVIDER'S STATEMENT (Please Print or Type)
THE HEALTH CARE PROVIDER'S STATEMENT MUST BE FILLED IN COMPLETELY. THE ATTENDING HEALTH CARE PROVIDER SHALL COMPLETE AND RETURN TO THE CLAIMANT WITHIN SEVEN (7) DAYS OF RECEIPT OF THIS FORM. For item
1. Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI: |
|
|
||||||||||
2.Gender: |
Male |
Female |
|
3. Date of Birth: |
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
4. Diagnosis/Analysis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnosis Code: |
|
|
|
|
|
|
|
|
|
|||||||||||
|
a. Claimant's symptoms: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
b. Objective findings: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Claimant hospitalized?: |
Yes |
No |
From: |
|
|
|
/ |
|
|
/ |
|
|
To: |
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
6. Operation indicated?: |
Yes |
No |
a. Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Date |
/ |
|
/ |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
ENTER DATES FOR THE FOLLOWING |
|
|
|
|
|
|
|
|
|
|
MONTH |
|
|
|
|
|
|
DAY |
|
|
|
|
YEAR |
|
||||||||||||||||||||
a Date of your first treatment for this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
b.Date of your most recent treatment for this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
c. Date Claimant was unable to work because of this disability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
d.Date Claimant will again be able to perform work (Even if considerable question |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
exists, estimate date. Avoid use of terms such as unknown or undetermined.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
e.If pregnancy related, please check box and enter the date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
estimated delivery date OR |
actual delivery date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
8. In your opinion, is this disability the result of injury arising out of and in the course of employment or occupational disease?:
|
Yes |
No If "Yes", has Form |
Yes |
No |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
I certify that I am a: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
(Physician, Chiropractor, Dentist, Podiatrist, Psychologist, |
Licensed or Certified in the State of |
|
|
License Number |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Health Care Provider's Printed Name |
|
|
Health Care Provider's Signature |
|
|
|
Date |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Health Care Provider's Address |
|
|
|
|
|
|
|
Phone # |
|||||||
IMPORTANT NOTICE TO CLAIMANT - READ THESE INSTRUCTIONS CAREFULLY
PLEASE NOTE: Do not date and file this form prior to your first date of disability. In order for your claim to be processed, Parts A and B must be completed.
1.If you are using this form because you became disabled while employed or you became disabled within four (4) weeks after termination of employment, your completed claim should be mailed within thirty (30) days of your first date of disability to your employer or your last employer's insurance carrier. You may find your employer's disability insurance carrier on the Workers' Compensation Board's website, www.wcb.ny.gov, using Employer Coverage Search.
2.If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim MUST be mailed to: Workers' Compensation Board, Disability Benefits Bureau, PO Box 9029, Endicott, NY
If you do not receive a response within 45 days or if you have questions about your disability benefits claim, please call your employer's insurance carrier. For general information about disability benefits, please visit www.wcb.ny.gov or call the Board's Disability Benefits Bureau at (877)
Notification Pursuant to the New York Personal Privacy Protection Law (Public Officers Law Article
HIPAA NOTICE - In order to adjudicate a workers' compensation claim or disability benefits claim, WCL
Disclosure of Information: The Board will not disclose any information about your case to any unauthorized party without your consent. If you choose to have such information disclosed to an unauthorized part, you must file with the Board an original signed Form
An employer or insurer, or any employee, agent, or person acting on behalf of an employer or insurer, who KNOWINGLY MAKES A FALSE STATEMENT OR REPRESENTATION as to a material fact in the course of reporting, investigation of, or adjusting a claim for any benefit or payment under this chapter for the purpose of avoiding provision of such payment or benefit SHALL BE GUILTY OF A CRIME AND SUBJECT TO SUBSTANTIAL FINES AND IMPRISONMENT.
| Fact Name | Description |
|---|---|
| Form Identification | The form in question is identified as DB-450 (1-20), indicating its version or edition. |
| Purpose | It serves as a Notice and Proof of Claim for Disability Benefits in New York State. |
| Submission Requirement | Claimants must answer all questions in Part A and questions 1 through 3 in Part B to avoid processing delays. |
| Health Care Provider's Involvement | Part B on page 2 must be completed by the claimant's health care provider to provide medical evidence of the disability. |
| Claimant Information | Part A requires detailed information from the claimant, including personal and employment details, and the nature of the disability. |
| Governing Law | The form is governed by New York State law, particularly referencing the New York Workers' Compensation Law (WCL) §§ 20 and 142 for its authority and purpose. |
| Privacy Notice | Includes notices under the New York Personal Privacy Protection Law and the Federal Privacy Act of 1974 regarding the claimant's personal information and social security number. |
Filing the DB-450 Disability Benefits form is a critical step in obtaining disability benefits in New York State. This form is necessary for documenting and proving your disability to access the benefits you're entitled to. Understanding the sections and specific requirements of the form ensures that your submission is complete and processed promptly, reducing delays in receiving support.
Here are the steps to filling out the DB-450 form:
Important: The DB-450 form requires timely submission to ensure prompt processing of your claim. Be mindful of the submission deadlines and specific instructions relating to your circumstances. Additionally, always keep a copy of the filled-out form and any correspondence for your records.
Frequently Asked Questions about the DB-450 Disability Form
The DB-450 form is the official document used in New York State for individuals to file a claim for disability benefits. It serves as both a notice and proof of claim that must be completed by the claimant and their health care provider.
This form must be filled out by any individual in New York State who becomes disabled and seeks to claim disability benefits. Part A of the form is completed by the claimant, providing their personal information and details about their disability. Part B is filled out by the claimant's health care provider, offering medical evidence to support the claim.
If you became disabled while employed, or within four weeks after your employment ended, you should mail the completed form within 30 days from the first day of disability to your employer or their insurance carrier. If you became disabled after being unemployed for more than four weeks, the form must be mailed directly to the Workers' Compensation Board's Disability Benefits Bureau at the specified address.
Leaving parts of the DB-450 form incomplete can delay the processing of your claim. It's important to answer all questions in Part A and the required questions in Part B to avoid delays. Health care providers must also complete their section of the form fully and return it to the claimant promptly.
No, you should not fill out and file this form before your disability begins. The form must be filled out based on the actual period of disability. Submitting the form prematurely can result in your claim being processed incorrectly.
If you are receiving or claiming other benefits such as unemployment benefits, paid family leave, workers’ compensation, or long-term disability benefits under the Federal Social Security Act, you must indicate this on the form. Providing false information or failing to disclose other benefits can affect your eligibility for disability benefits.
For further assistance or if you have questions not covered by this FAQ, you can visit www.wcb.ny.gov or call the Board's Disability Benefits Bureau.
When filling out the DB-450 Disability Benefits form, it's crucial to provide accurate and complete information to avoid delays in processing or potential denial of benefits. However, individuals commonly make several mistakes while completing this form. Recognizing and avoiding these errors can help ensure a smoother process in claiming disability benefits.
In addition to avoiding these common mistakes, it's also advisable to double-check the form for accuracy and completeness before submitting it. This extra step can help ensure that the claim is processed as efficiently as possible.
Filing the DB-450 Notice and Proof of Claim for Disability Benefits is a crucial first step for individuals in New York State to receive their disability benefits promptly. However, this form seldom stands alone in the application process. Other forms and documents often accompany the DB-450, each serving its own unique purpose in ensuring the claim is processed accurately and efficiently.
While the DB-450 form is the cornerstone of applying for disability benefits in New York State, these accompanying forms and documents play vital roles in painting a complete picture of the claimant’s situation. By thoroughly compiling and submitting the necessary paperwork, claimants can avoid delays and ensure a smooth processing of their disability benefits claim.
The DB-120.1: Notice of Compliance – Disability Benefits form parallels the DB-450 form, as both are designed for New York State, focusing on disability due to employment. The former is for employers to display compliance with disability benefits law, while the latter is a direct claim form for individuals experiencing a disability. Both necessitate precise employer and employee information and engage with New York's specific disability benefits structure.
The Form SS-5, Application for a Social Security Card, shares similarities with the DB-450 form as both require detailed personal identification information, such as social security numbers, birth dates, and contact information. Each form plays a distinct role in the provision of benefits or services from the government, focusing on the individual's needs and rights within the system.
The WH-380-E, Certification for Serious Health Condition form under the Family and Medical Leave Act (FMLA), is akin to the Part B of the DB-450 form. Both involve healthcare providers detailing the nature and extent of an individual's health condition, albeit for different reasons—FMLA for leave purposes and DB-450 for disability benefits.
The W-4 form, Employee's Withholding Certificate, though primarily used for tax withholding purposes, shares the necessity of collecting accurate employee information for administrative purposes with the DB-450. It emphasizes the importance of precise, personal information in effectively managing benefits and obligations.
The Workers' Compensation Claim Form (WC-100), like the DB-450, collects detailed information on the nature of an injury or illness, the circumstances around its occurrence, and employment details. Both forms are crucial for individuals seeking out benefits due to work-related incidents.
The UB-04 form, used for hospital billing, may not directly correlate to disability claims but is similar to the health care provider's segment of the DB-450. Both require diagnoses, treatment details, and provider information, aimed at facilitating payment or benefits for health-related issues.
Form I-9, Employment Eligibility Verification, while fundamentally designed for verifying work eligibility in the U.S., bears commonality with the DB-450 in the gathering of personal and employment information. Both forms are integral to regulatory compliance and personal identity verification in the context of employment.
When filling out the DB-450 Disability Form, consider the following guidelines to ensure a smooth processing of your claim:
By following these guidelines, you can help ensure that your DB-450 Disability Form is processed efficiently and without unnecessary delays.
There are several common misunderstandings about the DB-450 Disability Form, a crucial document for claiming disability benefits in New York State. Clarifying these misconceptions can help claimants navigate the process more effectively.
This is not correct. The form should only be dated and filed after the first day of disability to ensure the claim is processed accurately and promptly.
While the claimant must complete a significant portion of the form, healthcare providers are responsible for filling out Part B. This section requires professional medical input regarding the claimant's condition and prognosis.
Providing your Social Security number is actually voluntary. Omitting it won’t result in a denial of your claim or reduced benefits, as the form's instructions explicitly state there is no penalty for not providing this information.
Submission of the form starts the claim process, but benefits are subject to approval based on the provided evidence and verification by the employer or insurance provider. Claims can be delayed if the form is filled out incorrectly or incompletely.
Where to send your completed form depends on your employment status at the time of disability onset. Newly unemployed claimants send it to a specific address, while those still employed should send it to their employer or the employer’s insurance carrier. Guidance on this is clearly provided in the form's instructions.
The form inquires whether you are receiving other types of benefits to ensure proper coordination and determination of eligibility, but receiving certain benefits does not automatically disqualify you from receiving disability benefits.
Understanding these nuances is vital to navigating the process of filing a disability claim using the DB-450 form accurately and effectively.
When preparing to fill and submit the DB-450 Disability form, individuals navigating the complexities of disability benefits within New York State should pay mindful attention to several critical aspects. These facets are designed to streamline the process, ensuring that the pursuit of benefits does not become bogged down by preventable errors or omissions. Here are the key takeaways:
Finally, claimants are urged to provide accurate and truthful information throughout the form. Any attempt to submit false statements or representations in connection with the claim may lead to severe legal repercussions including fines and imprisonment. This underscores the government's commitment to integrity and fairness in the administration of disability benefits.
1750 Pdf - The form is a vital document for audit and inspection purposes, providing clear evidence of shipped items and quantities.
Resale Number California - The document serves as a commitment not to use the bought items for personal purposes before resale.
Wv Sales and Use Tax Form - The inclusion of high technology business services and educational software indicates a recognition of modern business operations and their eligibility for tax-exempt status under certain conditions.