Free DD 2870 PDF Template
Free DD 2870 PDF Template
For individuals navigating the complexities of accessing medical records within the military health system, the DD 2870 form serves as a critical tool. This document, designed for use by service members, veterans, and their dependents, streamlines the process of requesting and authorizing the release of medical or dental treatment records held by military medical facilities. Understanding the intricacies of the DD 2870 form unlocks the ability to efficiently manage one’s healthcare documentation, ensuring that those entitled to care or overseeing the care of others can readily obtain necessary records. The form emphasizes privacy and compliance with regulations on information sharing, highlighting the importance of informed consent in the medical field. Its proper completion and submission are key to facilitating smooth communication between healthcare providers, patients, and authorized entities, making it a cornerstone in the pursuit of coordinated and effective healthcare services within the Department of Defense's vast medical system.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
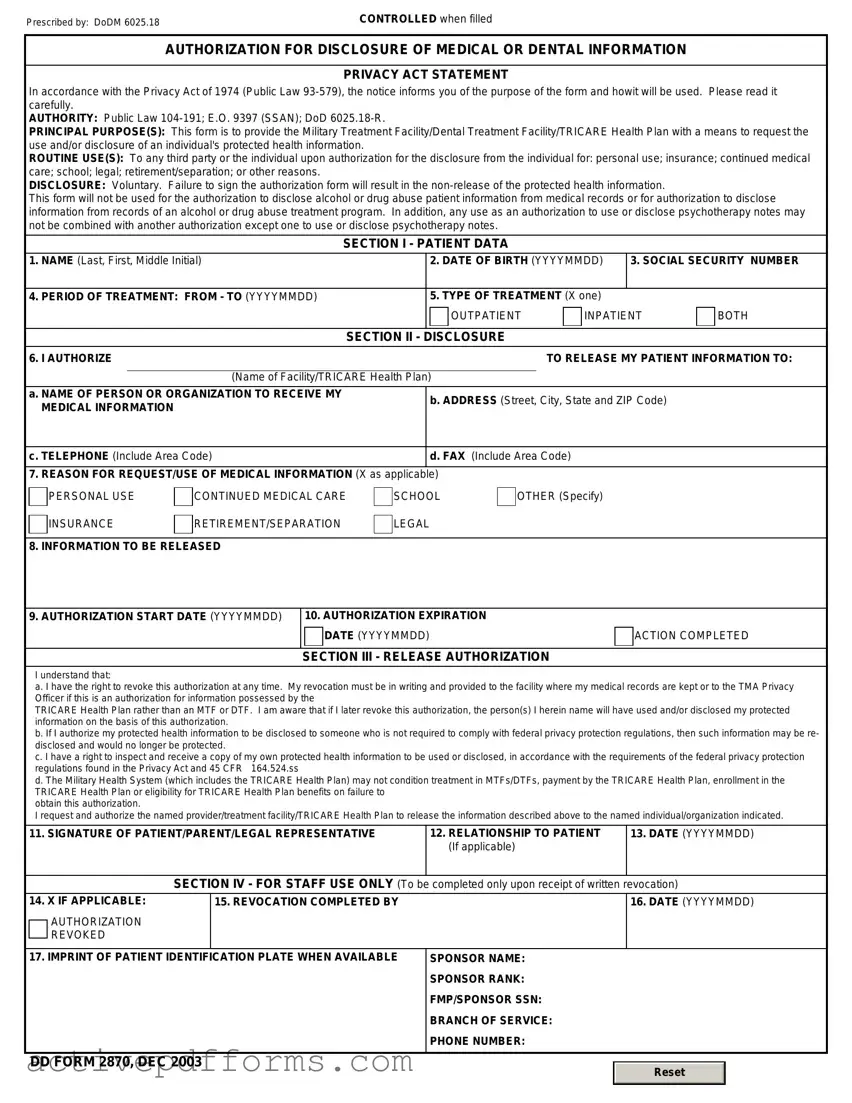
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
| Fact | Description |
|---|---|
| Name of the Form | DD Form 2870, "Authorization for Disclosure of Medical or Dental Information" |
| Purpose | Used to request the release of medical or dental records from military facilities |
| Who Uses It | Individuals seeking access to their own medical records or those authorized to receive someone else's records |
| Where It's Used | Primarily used within the Department of Defense and its medical facilities |
| Information Required | Personal identification information, the specifics of the information being requested, and the purpose of the request |
| Privacy Concerns | Handled with strict compliance to HIPAA (Health Insurance Portability and Accountability Act) regulations to protect individuals' medical information |
| Processing Time | Can vary; it's recommended to submit requests well in advance of when the records are needed |
| No State-Specific Versions | This form is federally standardized and does not have state-specific versions |
| Governing Law(s) | Federal laws, mainly HIPAA, govern the use and processing of this form |
Filling out the DD 2870 form is a necessary process for those seeking to authorize the release of medical or dental records. This form is crucial for ensuring that patient information is shared securely and in compliance with privacy laws. Completing this form accurately is essential for facilitating the prompt and correct handling of medical records. The steps outlined below are designed to assist individuals in filling out the form correctly, ensuring that their information is handled appropriately.
After completing the DD 2870 form, it should be submitted to the appropriate medical records office where the records are held. This can usually be done in person, via mail, or in some cases, through secure electronic submission methods. Once the form is processed, the records will be prepared and sent to the specified recipient within the timeframe outlined by the medical facility's policy. It's important to follow up if confirmation of receipt is not received within the expected period.
What is the DD 2870 form used for?
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, is primarily utilized to grant permission for the release of an individual's medical or dental records. It is often used by military personnel, veterans, and their dependents. The form serves as a written consent, allowing healthcare providers to share the specified health information with designated parties, such as insurance companies, healthcare providers, or legal representatives.
Who needs to complete the DD 2870 form?
This form must be completed by individuals or their authorized representatives who are seeking to have medical or dental records released to third parties. It is applicable to service members, their families, and other beneficiaries receiving care within the military health system. Completing the form accurately ensures that privacy regulations are upheld while allowing necessary information to be shared for the purposes specified by the requester.
Where should the completed DD 2870 form be submitted?
Once filled out, the form should be submitted to the medical or dental facility that holds the records you wish to have released. Each facility has its own process for handling these requests, so it is advisable to contact the specific facility directly to inquire about the proper submission method, whether it be in person, by mail, or through secure electronic means, if available.
What information is required to fill out the DD 2870 form?
To properly complete the form, individuals must provide detailed information including, but not limited to, the patient's full name, date of birth, Social Security Number (SSN) or DoD Identification Number, the specific records being requested, the purpose of the disclosure, and the name and address of the recipient of the information. Additionally, the form must be signed and dated by the patient or their legal representative. This ensures that the request is valid and that consent has been officially given for the disclosure.
Not checking the correct authorization box often leads to confusion about what type of information is being requested. This mistake can significantly delay processing because it's crucial to specify whether the request is for medical records, dental records, or both.
Forgetting to sign and date the form is a common oversight. Without a signature and date, the form is not legally binding, meaning that the authorities cannot legally release the information requested. This oversight can result in a complete halt in the processing of the request.
Incomplete patient information is a frequent error. Every field related to the patient's identity, including full name, Social Security Number (SSN), and date of birth, must be accurately filled. Missing or incorrect details can prevent the identification of the correct record, leading to significant delays.
Many individuals mistakenly provide insufficient information about the record(s) being requested. Details such as the type of documents needed and the specific dates of service help in locating the exact information needed. Vague requests can result in incomplete fulfillment of the request.
Another common mistake is failure to specify the purpose of the request. Whether the records are needed for personal use, legal matters, or medical continuity of care, stating the purpose helps in processing the request efficiently and ensures that the information provided is relevant.
Finally, incorrectly addressing the form to the wrong department or facility can cause unnecessary delays. It's crucial to research and confirm the correct address and department to which the DD 2870 form should be sent to ensure it reaches the right hands without any delays.
In the context of managing healthcare records and permissions within the United States military system, the DD 2870 form, or Authorization for Disclosure of Medical or Dental Information, plays a pivotal role. It is designed to allow service members to authorize the release of their medical records to designated parties. This process often requires additional documentation to ensure accurate, legal, and effective handling of personal health information. Understanding these accompanying documents can provide a more comprehensive grasp of the healthcare authorization process within military contexts.
The compilation of these documents, alongside the DD 2870, outlines a framework within which individuals can navigate their healthcare information seamlessly across military and civilian lines. This network of forms creates a structured path for the authorization, release, and utilization of medical information, safeguarding the individual's rights while ensuring compliance with both federal and military regulations. Understanding each document’s role and function supports service members and veterans in managing their health care more effectively and ensures their privacy and preferences are respected.
Health Insurance Portability and Accountability Act (HIPAA) Authorization Form: Similar to the DD 2870, the HIPAA Authorization Form allows individuals to grant third parties access to their personal health information. Both documents ensure confidentiality and compliance with federal privacy regulations.
Medical Records Release Form: Often used in healthcare settings, this form parallels the DD 2870 by enabling patients to authorize the disclosure of their medical records to specified recipients for various reasons, including treatment and insurance purposes.
Power of Attorney (POA) for Healthcare: This legal document allows an individual to appoint someone else to make healthcare decisions on their behalf, somewhat similar to the DD 2870, which authorizes access to medical information, potentially influencing decisions about care.
Informed Consent Form: Used in medical and research settings, it shares similarities with the DD 2870 by requiring individuals to acknowledge understanding and agreement to procedures or treatment, including the release of medical information for specific purposes.
Family Educational Rights and Privacy Act (FERPA) Release Form: While FERPA focuses on educational records, it is akin to the DD 2870 in its function to authorize the release of private information to third parties, adhering to federal privacy standards.
Third-Party Authorization Form for Financial Accounts: This form allows individuals to grant third parties access to their banking or financial information, similar to the DD 2870 authorizing access to medical records but within a financial context.
Consent for Treatment Form for Minors: This document enables parents or guardians to authorize medical treatment for underage individuals, sharing similarities with the DD 2870 by necessitating consent for the release and sharing of medical information concerning minors.
Release of Information (ROI) Form in Social Services: Used within social services agencies to authorize the disclosure of personal information to third parties, the ROI Form helps in managing an individual's case, similar to how the DD 2870 facilitates healthcare management through information sharing.
Advance Directive Forms: These documents allow individuals to outline their preferences for medical treatment and end-of-life care, indirectly related to the DD 2870 as both involve aspects of healthcare preferences and the sharing of sensitive information.
Employment Background Check Authorization Form: This form authorizes employers to conduct background checks on potential hires, including accessing personal information. It is similar to the DD 2870, which involves consent for accessing specific types of personal records, albeit for different purposes.
The DD 2870 form, better known as the Authorization for Disclosure of Medical or Dental Information, is crucial in managing the confidentiality and sharing of medical records. Given the sensitivity of the data involved, it's important to handle this form with the utmost care. Below are ten essential do's and don'ts to keep in mind when completing the DD 2870 to ensure the process is both smooth and secure.
Do:Read the instructions carefully. Before you start filling in the form, ensure you understand every requirement to avoid any mistakes.
Verify the information of the individual whose records are being requested, including their full name, Social Security Number, and other vital details, to ensure accuracy.
Clearly identify the purpose of the request. Specify why you need the medical or dental information to avoid any confusion or processing delays.
Include the name and address of the person or organization authorized to receive the medical information. This step is critical to ensure the records are sent to the correct destination.
Sign and date the form. A signature is required to process the document, and dating it helps establish the relevance of the authorization.
Leave any sections incomplete. Every part of the DD 2870 form requires your attention to provide a clear and lawful authorization.
Forget to specify any restrictions. If you wish to limit what information is shared, clearly outline these restrictions in the appropriate section of the form.
Use unclear or vague language. Be as precise as possible to avoid any misunderstandings or errors in processing your request.
Overlook the need for a witness or notary, if required. Some states or situations may require a witness or notarial seal to validate the authorization.
Ignore the expiration date of your authorization. Make sure to state when the authorization ends to protect the privacy of the individual’s information after the purpose of the request has been served.
Correctly completing the DD 2870 form is a responsibility that protects individuals' medical privacy and ensures information is shared according to their wishes. Being diligent and thorough in this process reinforces trust and compliance with federal privacy laws.
The DD 2870 form, or the Authorization for Disclosure of Medical or Dental Information, is surrounded by various misconceptions. These misunderstandings can lead to confusion about the form's purpose, the process of completing it, and its implications. Here, we aim to clarify some of these common misconceptions.
It grants access to all medical records indefinitely. The DD 2870 form does not give indefinite access to medical records. It allows for the disclosure of specific medical or dental information within a timeframe specified by the individual granting the permission.
It's only for military personnel. While commonly associated with the military, the form can also be used by dependents and other individuals who receive care through military health services to authorize the release of their medical information.
Verbal consent is just as effective. Verbal consent cannot replace the DD 2870. Written permission through this form is necessary for the release of medical or dental records in compliance with privacy regulations.
Any medical provider can access records with this form. The DD 2870 form specifically designates who is authorized to receive the information. The individual filling out the form must clearly specify the recipient, ensuring that only those intended can access the records.
It's a complicated process. Completing the DD 2870 form is straightforward. It requires basic information about the individual, the type of records to be released, to whom, and the purpose of the disclosure.
Once signed, it cannot be revoked. The individual who authorizes the release of information can revoke the consent at any time. This revocation must be done in writing.
It covers all types of disclosures. The DD 2870 is specifically for the disclosure of medical or dental records. It does not cover other types of personal information such as educational or financial records.
There's no need to specify the type of information being released. The form requires the individual to specify the type of medical or dental information to be disclosed. This ensures that only relevant information is shared.
It automatically renews. The DD 2870 does not have an automatic renewal feature. If continued access to medical or dental records is needed after the original authorization expires, a new form must be completed.
It allows for unrestricted sharing of information. The form includes provisions to protect the individual's privacy. It only permits the sharing of information with parties specified by the individual filling out the form and for the purpose stated in the authorization.
Understanding these key aspects of the DD 2870 form can ensure that individuals are better informed about their privacy rights and the process of authorizing the release of medical or dental information.
Understanding the DD 2870 form is critical for those seeking access to medical records or authorizing disclosure of medical information. This form, utilized within the Department of Defense, serves as a controlled pathway for individuals to manage the confidentiality and sharing of personal medical records. Here are key takeaways about filling out and using the DD 2870 form:
By following these guidelines, individuals can effectively navigate the process of accessing or sharing their medical records through the DD 2870 form, ensuring their privacy is maintained and their needs are accurately addressed.
Free Trailer Inspection Checklist - Includes a dedicated section for detailed comments, allowing inspectors to note specific concerns or damages.
Vtr 275 - Guides on the application submission process including mailing instructions and documentation.