Free Ld 0274 PDF Template
Free Ld 0274 PDF Template
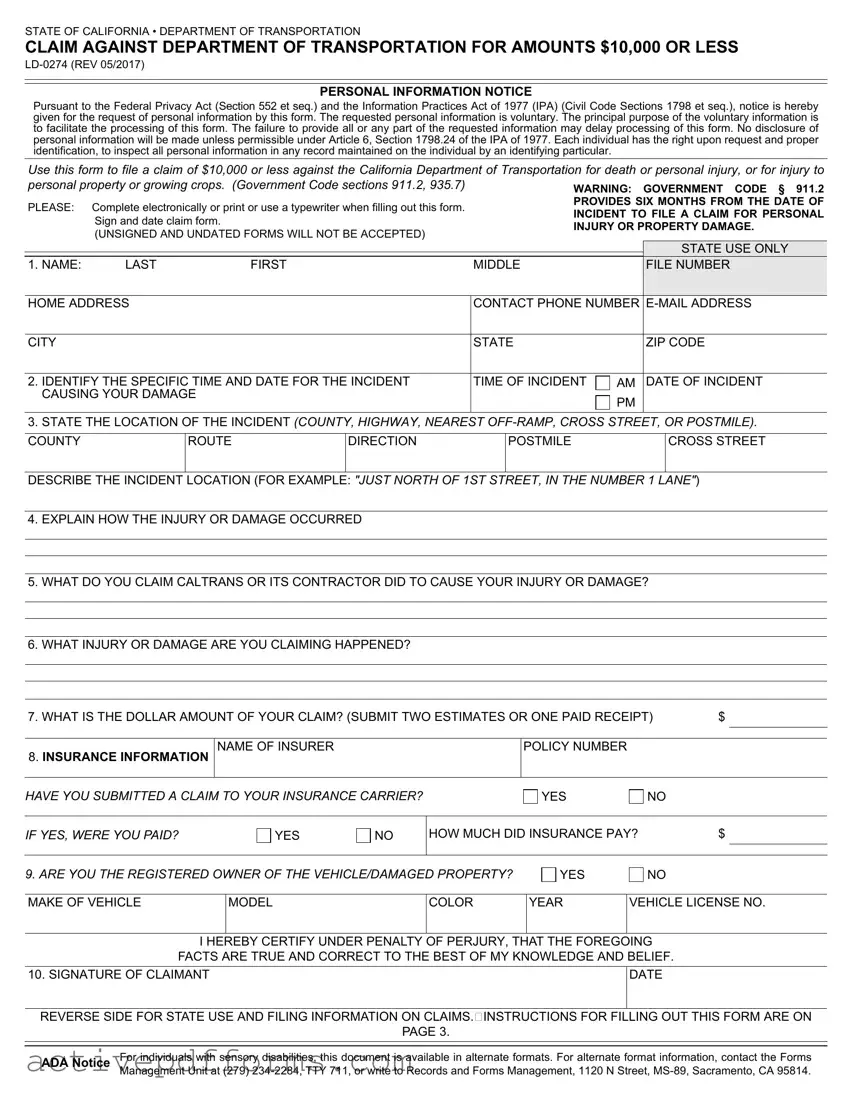
Navigating through the legal protocol for filing a claim against the Department of Transportation in California for damages of $10,000 or less can seem overwhelming, but understanding the LD-0274 form is a critical step towards a streamlined process. This form serves as the official document to request compensation for personal injury, property damage, or damage to growing crops due to the actions or negligence of the California Department of Transportation (Caltrans) or its contractors. Detailed in nature, it requires personal information in compliance with both the Federal Privacy Act and the Information Practices Act of 1977, ensuring confidentiality and the right to inspect personal information records. Beyond basic details, the form mandates a thorough account of the incident, including the precise time and location, a clear explanation of the injuries or damages incurred, and a specific claim against Caltrans' actions leading to said damages. Additionally, claimants are urged to provide financial documentation supporting their claim amount and disclose insurance information, which plays a vital role in the processing and evaluation of the claim. Security measures such as requiring a signature and adherence to filing deadlines underscore the seriousness and formal nature of the claim process. With a clear understanding and careful completion of the LD-0274 form, individuals seeking reparations have a structured path to potentially receiving compensation for their grievances.
STATE OF CALIFORNIA • DEPARTMENT OF TRANSPORTATION
CLAIM AGAINST DEPARTMENT OF TRANSPORTATION FOR AMOUNTS $10,000 OR LESS
PERSONAL INFORMATION NOTICE
Pursuant to the Federal Privacy Act (Section 552 et seq.) and the Information Practices Act of 1977 (IPA) (Civil Code Sections 1798 et seq.), notice is hereby given for the request of personal information by this form. The requested personal information is voluntary. The principal purpose of the voluntary information is to facilitate the processing of this form. The failure to provide all or any part of the requested information may delay processing of this form. No disclosure of personal information will be made unless permissible under Article 6, Section 1798.24 of the IPA of 1977. Each individual has the right upon request and proper identification, to inspect all personal information in any record maintained on the individual by an identifying particular.
Use this form to file a claim of $10,000 or less against the California Department of Transportation for death or personal injury, or for injury to
personal property or growing crops. (Government Code sections 911.2, 935.7) |
WARNING: GOVERNMENT CODE § 911.2 |
|||||
PLEASE: |
Complete electronically or print or use a typewriter when filling out this form. |
PROVIDES SIX MONTHS FROM THE DATE OF |
||||
INCIDENT TO FILE A CLAIM FOR PERSONAL |
||||||
|
Sign and date claim form. |
|
||||
|
|
INJURY OR PROPERTY DAMAGE. |
||||
|
(UNSIGNED AND UNDATED FORMS WILL NOT BE ACCEPTED) |
|||||
|
|
|
|
|||
|
|
|
|
|
STATE USE ONLY |
|
|
|
|
|
|
||
1. NAME: |
LAST |
FIRST |
MIDDLE |
|
FILE NUMBER |
|
|
|
|
|
|||
HOME ADDRESS |
|
CONTACT PHONE NUMBER |
||||
|
|
|
|
|
|
|
CITY |
|
|
STATE |
|
ZIP CODE |
|
|
|
|
|
|||
2. IDENTIFY THE SPECIFIC TIME AND DATE FOR THE INCIDENT |
TIME OF INCIDENT |
AM |
DATE OF INCIDENT |
|||
CAUSING YOUR DAMAGE |
|
|
PM |
|
||
|
|
|
|
|
||
3.STATE THE LOCATION OF THE INCIDENT (COUNTY, HIGHWAY, NEAREST
COUNTY |
ROUTE |
DIRECTION |
POSTMILE |
CROSS STREET |
DESCRIBE THE INCIDENT LOCATION (FOR EXAMPLE: "JUST NORTH OF 1ST STREET, IN THE NUMBER 1 LANE")
4.EXPLAIN HOW THE INJURY OR DAMAGE OCCURRED
5.WHAT DO YOU CLAIM CALTRANS OR ITS CONTRACTOR DID TO CAUSE YOUR INJURY OR DAMAGE?
6.WHAT INJURY OR DAMAGE ARE YOU CLAIMING HAPPENED?
7. WHAT IS THE DOLLAR AMOUNT OF YOUR CLAIM? (SUBMIT TWO ESTIMATES OR ONE PAID RECEIPT) |
$ |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
8. INSURANCE INFORMATION |
NAME OF INSURER |
POLICY NUMBER |
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
YES |
NO |
HOW MUCH DID INSURANCE PAY? |
$ |
YES |
NO |
MAKE OF VEHICLE
MODEL
COLOR
YEAR
VEHICLE LICENSE NO.
10. SIGNATURE OF CLAIMANT
DATE
ADA Notice |
For individuals with sensory disabilities, this document is available in alternate formats. For alternate format information, contact the Forms |
|
Management Unit at (279) |
STATE OF CALIFORNIA • DEPARTMENT OF TRANSPORTATION
CLAIM AGAINST DEPARTMENT OF TRANSPORTATION FOR AMOUNTS $10,000 OR LESS
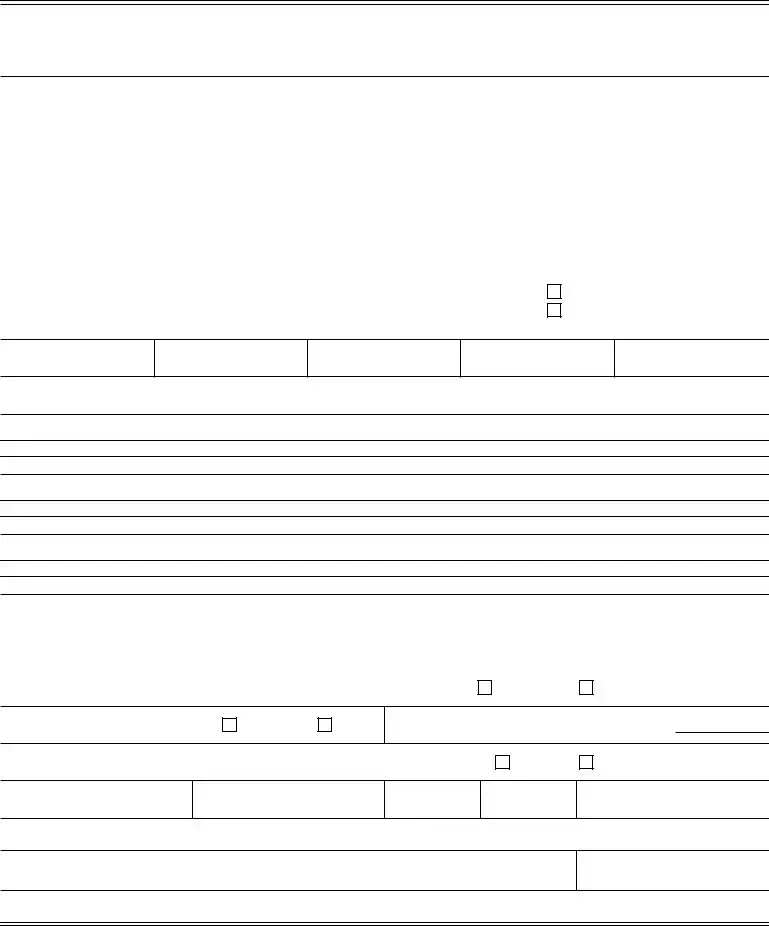
FOR STATE USE ONLY (BELOW)
DATE CLAIM RECEIVED |
REVIEWED BY: DISTRICT CLAIMS OFFICER |
|
AMOUNT APPROVED $ |
||||
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
TORT FUND/ |
CONTRACTOR |
DENIED |
||||
RESPONSIBILITY |
CONTRACT CONTINGENCY |
RESPONSIBILTY |
DENIAL DATE |
||||
|
|
|
|
|
|
|
|
DISTRICT
LOCATION CODING
COUNTYROUTE
POSTMILE
COST CODING
DEPARTMENT |
FUND |
|
UNIT |
OBJECT |
PROJECT NUMBER |
|
PHASE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ITEM |
|
|
CHAPTER |
STATUTES |
|
FISCAL YEAR |
SCHEDULE NUMBER |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCOUNTING OFFICER SIGNATURE |
|
DATE |
|||
|
|
|
|
|
|
|
|
|
|
FOR CLAIMS TEN THOUSAND DOLLARS ($10,000) OR LESS
Select District
Address
FOR CLAIMS OVER TEN THOUSAND DOLLARS ($10,000)
You must file a claim with the Government Claims Program in West Sacramento, California.
If you have any questions about claims of more than ten thousand dollars ($10,000), contact:
Government Claims Program
Office of Risk and Insurance Management
Department of General Services
P.O. Box 989052, MS 414
West Sacramento, CA
Phone:
Website: http://www.dgs.ca.gov/orim/Programs/GovernmentClaims.aspx
The fact that this brief statement of the initial procedure to be followed in submitting a claim against the State of California, or against any of the State of California's subdivisions, departments, divisions, agencies, officers, employees, agents, or directors, has been furnished to you or that an investigation of any claim is undertaken is not to be taken as an admission of liability in any respect on the part of the State of California, or by any of the State of California's subdivisions, departments, divisions, agencies, officers, employees, agents, or directors, nor is the fact that this informational statement has been furnished to you to be construed as a waiver of any requirements imposed by the law or of any defense which may be available to the State of California or to any of the State of California's subdivisions, departments, divisions, agencies, officers, employees, agents, or directors, in connection with any claim that may be filed.
ADA Notice |
For individuals with sensory disabilities, this document is available in alternate formats. For alternate format information, contact the Forms |
|
Management Unit at (279) |

STATE OF CALIFORNIA • DEPARTMENT OF TRANSPORTATION
CLAIM AGAINST DEPARTMENT OF TRANSPORTATION FOR AMOUNTS $10,000 OR LESS
INSTRUCTIONS FOR FORM
Please note that failure to complete all sections of the claim form may delay the processing of your claim or result in the return of your claim.
1.Claimant's Name and Contact Information: State the full name, mailing address,
2.Date and Time When the Injury/Damage First Occurred: State the exact month, day, year, and time of the incident giving rise to the claim.
3.Location of Incident: Specify the county, highway number, direction of travel, post mile, nearest exit(s),
4.How Your Injury/Damage Occurred: Provide complete details about what happened to cause your injury/damages. If you need more space, you may attach additional pages.
5.What Do You Claim Caltrans or Its Contractor Did to Cause Your Injury or Damage? State in detail all facts in support of your claim. Identify all persons or entities involved and why you believe Caltrans or its contractor is liable. If applicable, provide the name of the Caltrans employee or contractor, and the State of California vehicle license plate/ID number. If you need more space, you may attach additional pages.
6.What Injury or Damage Are You Claiming Happened? Specify the exact injury or damage for which you are claiming, including all alleged injuries, property damage, and/or loss. If you need more space, you may attach additional pages. You can attach photographs and any additional supporting documents. If you do, be sure the photographs show the damage and its size relative to the vehicle. More than one photograph provides more information to assist the evaluation of your claim.
7.What Is the Dollar Amount of Your Claim? State the total dollar amount for which you are claiming. Leaving the dollar amount blank will result in your claim being deemed incomplete, and your claim will be returned without further action. Please submit two (2) written estimates and/or one (1) paid receipt for all damages claimed. If you are submitting proof of payment, copies of credit card statements or copies of the front and back of cancelled checks are required. Invoices will not be accepted as actual proof of payment. All invoices must list the claimant's name and vehicle license plate number, vendor's letterhead, and an itemized list of repairs. Caltrans will not accept quotes retrieved from the internet.
8.Insurance Information: State the name of your insurer and policy number. If you have been reimbursed by your insurance company, you may not be eligible for compensation.
9.Are You the Registered Owner of the Vehicle/Damaged Property? Only the registered owner may file a claim for damage to a vehicle or property. Be sure to provide all vehicle information, including a copy of the vehicle's registration.
10.Signature of Claimant: Please sign and date the claim form. Caltrans does not accept claim forms without an original signature. Faxed or photocopied claim forms will not be accepted.
Mailing Completed Form: The completed form must be mailed to the District Claims Office assigned to the county in which your injury/ damages occurred. To determine the proper District Claims Office to which you should mail your completed form, you can use the map on the website and click on the county. The website map will show the District Claims Office responsible for that county, including its address and telephone number. You can then use the drop down menu on page 2 of this form to automatically fill in the address for the appropriate District Claims Office. If you have any questions about the location where your injury/damages occurred, you can contact any District Claims Office.
If your claim is over ten thousand dollars ($10,000.00), you must file a different form with the Government Claims Program WITHIN 6 MONTHS OF THE DATE OF INCIDENT. A claim form may be obtained by contacting the Government Claims Program at:
Government Claims Program
Office of Risk and Insurance Management Department of General Services
P.O. Box 989052, MS 414
West Sacramento, CA
The claim form may also be downloaded from the Government Claims Program website at:
http://www.dgs.ca.gov/orim/Programs/GovernmentClaims.aspx
The fact that this brief statement of the initial procedure to be followed in submitting a claim against the State of California, or against any of the State of California's subdivisions, departments, divisions, agencies, officers, employees, agents, or directors, has been furnished to you or that an investigation of any claim is undertaken is not to be taken as an admission of liability in any respect on the part of the State of California, or by any of the State of California's subdivisions, departments, divisions, agencies, officers, employees, agents, or directors, nor is the fact that this informational statement has been furnished to you to be construed as a waiver of any requirements imposed by the law or of any defense which may be available to the State of California or to any of the State of California's subdivisions, departments, divisions, agencies, officers, employees, agents, or directors, in connection with any claim that may be filed.
ADA Notice |
For individuals with sensory disabilities, this document is available in alternate formats. For alternate format information, contact the Forms |
|
Management Unit at (279) |
| Fact Name | Description |
|---|---|
| Form Purpose | The LD-0274 form is used to file a claim of $10,000 or less against the California Department of Transportation for death, personal injury, or for injury to personal property or growing crops. |
| Legal Basis | This form operates under the Government Code sections 911.2, 935.7. |
| Completion Guidelines | Claimants should complete the form electronically or use a typewriter, ensuring it is signed and dated, as unsigned and undated forms will not be accepted. |
| Filing Deadline | There is a six-month filing deadline from the date of the incident for personal injury or property damage claims, as specified by Government Code § 911.2. |
| Privacy Notice | The collection of personal information is governed by the Federal Privacy Act and the Information Practices Act of 1977, ensuring that disclosure is permissible only under specific conditions. |
| Documentation Required | Claimants must submit two estimates or one paid receipt for the damages claimed. Additional documentation, like photographs or police reports, can be attached to support the claim. |
| Accessibility | For individuals with sensory disabilities, alternative formats of the document are available upon request through the Forms Management Unit. |
After an incident involving the California Department of Transportation (Caltrans), knowing what steps to take next can be confusing. Filling out Form LD-0274 is necessary for claims against Caltrans for amounts $10,000 or less, concerning personal injury, property damage, or damage to growing crops. This process requires attention to detail and accuracy to ensure your claim is processed smoothly. Below are the steps to fill out the form accurately, which will help speed up the review process and move your claim forward.
Completing Form LD-0274 with accurate and comprehensive information is the first step in filing a claim for damages under $10,000 with the California Department of Transportation. Remember, claims should be filed promptly, keeping in mind that the deadline for submitting these documents is six months from the date of the incident. With the form filled out, you can look forward to the next part of the process, which might include further communication from Caltrans or the review of your claim.
Frequently Asked Questions about the LD-0274 Form
The LD-0274 form is used to file a claim of $10,000 or less against the California Department of Transportation (Caltrans) for death or personal injury, or for injury to personal property or growing crops. This form facilitates the processing of claims following incidents involving Caltrans or its contractors.
Individuals or entities looking to claim compensation for personal injury, property damage, or other losses of $10,000 or less resulting from an incident involving the California Department of Transportation or its contractors should complete this form. It is pertinent to those seeking a formal process to request reimbursement or damages directly related to Caltrans' operations or oversights.
The form can be completed electronically, by typewriter, or printed and filled out by hand. Once completed, it must be signed and dated, as unsigned and undated forms will not be accepted. The fully completed form should be submitted to the appropriate district address provided in the form instructions for amounts of $10,000 or less.
According to Government Code § 911.2, you have six months from the date of the incident to file a claim for personal injury or property damage using the LD-0274 form. Failing to submit within this timeframe could result in the forfeiture of your right to claim.
Key details required on the form include:
Additional evidence such as photographs, maps, and police reports (if available) can further support the claim.
If your claim exceeds $10,000, it must be filed with the Government Claims Program in West Sacramento, California. For guidance on claims over $10,000, contacting the Government Claims Program Office of Risk and Insurance Management at the Department of General Services is advisable. The LD-0274 form is strictly for claims of $10,000 or less.
Filling out the LD-0274 form to claim against the California Department of Transportation can seem straightforward, yet it's easy to make mistakes that can delay or even derail your claim. Here are seven common mistakes people make when completing this form:
Not providing complete contact information: Failing to fill out your full name, mailing address, email address, and contact phone numbers can lead to delays in processing your claim. It's crucial to ensure that all contact details are accurate and current.
Omitting the specific time and date of the incident: It’s essential to include the exact month, day, year, and time when the incident occurred. Vague or incomplete information makes it harder to investigate your claim.
Being vague about the incident location: Not specifying the county, highway number, direction of travel, postmile, nearest exits, cross-streets, or other helpful details can significantly slow down the claim process. A detailed description, or even a map, helps pinpoint the exact location of the incident.
Incomplete descriptions of how the injury or damage occurred: A thorough explanation of the events leading to the injury or damage is crucial. If necessary, attach additional pages to provide a complete account. This helps in understanding the circumstances and assessing liability.
Not detailing the actions leading to the claim: You must clearly state what you believe Caltrans or its contractor did to cause your injury or damage. Including names, state vehicle license plate or ID numbers, and specific actions or negligence can support your claim.
Leaving out descriptions of the injury or damage: It's important to specify all alleged injuries, property damage, and/or losses in detail. Attaching photographs and supporting documents can further strengthen your claim by providing visual evidence of the damage.
Omitting the dollar amount of the claim: Not stating the total dollar amount being claimed makes the claim incomplete. Providing two written estimates or one paid receipt is necessary to substantiate the amount requested.
Avoiding these mistakes can streamline the claim process, improving the chances that your claim will be processed promptly and efficiently. Remember, providing detailed and accurate information is key to a successful outcome.
When filing a claim against the California Department of Transportation using the LD-0274 form, it's often necessary to gather and complete additional documents to strengthen your case and ensure a thorough review. Here's a look at some of these key documents and why they're used alongside the LD-0274 form.
Preparing a comprehensive package, including the LD-0274 form and these supplementary documents, can significantly enhance the clarity and strength of your claim. Each piece of evidence plays a vital role in building a clear narrative of the incident and its repercussions, thereby facilitating a smooth review process. Remember that the ultimate goal is to present a well-documented case that accurately reflects the event and its impact on your life or property.
The Standard Form 95 is similar to the LD-0274 form as it is used to present claims against the federal government for property damage, personal injury, or death alleged to have been caused by the negligent or wrongful act of a federal employee. Like the LD-0274, it requires detailed information about the claimant, the incident, and damages sought.
Government Claims Program Application is also similar. Used for filing claims that exceed $10,000 against the State of California, this application, like the LD-0274, demands personal information, incident specifics, and the amount claimed. However, it is used for larger claims.
Small Claims Court Forms share similarities with the LD-0274, as they are utilized for seeking damages (usually under $10,000) due to personal injury or property damage. Both set-ups necessitate providing evidence, detail of the incident, and the valuation of damages.
The Notice of Claim Form used by city or county government entities parallels the LD-0274 in its requirement for claimants to detail incidents involving property damage or personal injury caused by municipal services or operations, detailing how the incident occurred and the requested compensation.
Demand Letter for Personal Injury or Property Damage often serves as a preliminary step before formal claims like LD-0274 are filed. Though less structured, it similarly outlines the incident, the damages incurred, and the compensation sought from the responsible party.
The Property Damage Report Form used by insurance companies mimics the LD-0274's purpose of documenting incidents leading to personal or property damage. It gathers claimant information, details of the incident, and an assessment of damages for insurance claims processing.
Incident Report Forms used within businesses or organizations for internal documentation of accidents or damage events share objectives with the LD-0274. These forms compile information on what happened, involved parties, and an estimate of damages or injuries to manage liability and insurance claims.
When filling out the LD-0274 form, a claim against the California Department of Transportation for amounts $10,000 or less, it is crucial to pay attention to both what you should and shouldn't do to ensure a smooth processing of your claim. Here are seven essential dos and don'ts:
By following these guidelines, you can ensure that your claim is filed correctly and improve the chances of a favorable outcome. Remember, attention to detail and adherence to the form's requirements are key to a successful claim process.
There are several misconceptions about the LD-0274 form used for filing claims against the California Department of Transportation for amounts $10,000 or less. Clarification of these misunderstandings can help individuals navigate the claims process more effectively.
Understanding these aspects of the LD-0274 form can significantly improve the accuracy and efficiency of filing a claim, ensuring individuals are better prepared and informed throughout the process.
When dealing with something as crucial as a claim against the Department of Transportation in California, particularly when this claim is for amounts $10,000 or less, navigating the LD-0274 form can seem daunting. However, understanding a few key points can simplify the process significantly, ensuring that your claim is not only filed correctly but also has the best chance of being processed smoothly and efficiently. Below is an overview of essential takeaways for filling out and using the LD-0274 form effectively:
By meticulous adherence to these guidelines, claimants can navigate the complexities of the LD-0274 form, effectively submitting their claims for consideration. Remember, while the process might seem intricate, each step is designed to ensure fairness and thoroughness in evaluating your claim against the California Department of Transportation.
Fire Department Pre Plan Example - Business and emergency contact information for key personnel promotes efficient communication during crises.
Truck Drivers Daily Run Sheet - Format for establishing a clear timeline of events and assigning duties for smooth operation.
What Is an Odometer Disclosure Statement - Facilitates an honest exchange of vehicle information, fostering trust in automotive transactions.