Free Medication Administration Record Sheet PDF Template
Free Medication Administration Record Sheet PDF Template
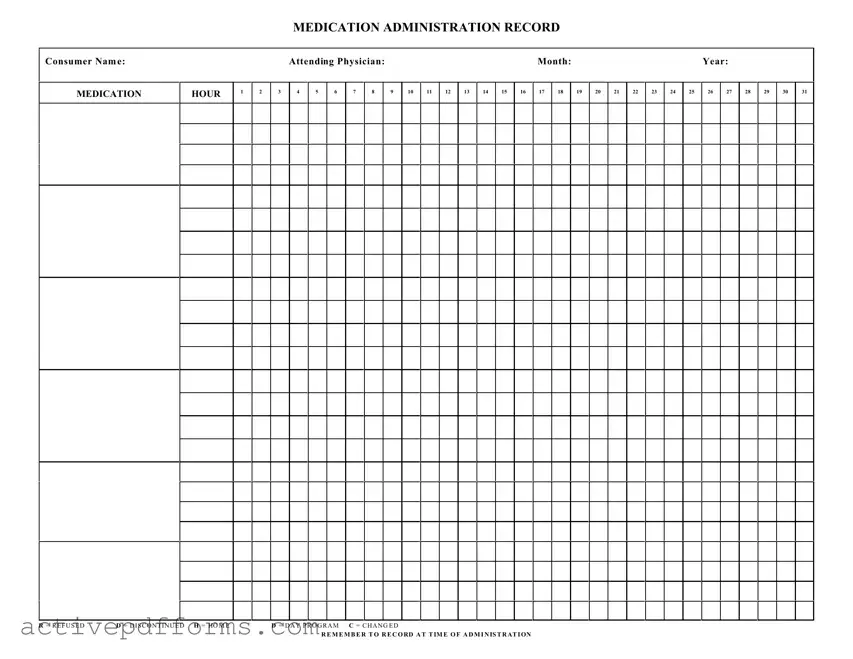
Ensuring that individuals receive their prescribed medications accurately and on time is critical for managing health conditions and promoting overall well-being. The Medication Administration Record Sheet form serves as an essential tool in this process, enabling caregivers and healthcare professionals to track the administration of medications to patients. This form contains key information, including the consumer's name, the medication hour—delineated into sections for each hour of the day—and spaces to note the attending physician's name, along with the month and year. It also includes specific codes such as "R" for refused, "D" for discontinued, and others indicating changes, home administration, or day program settings, making it versatile for various caregiving environments. Furthermore, it emphasizes the importance of recording each medication administration at the time it occurs, ensuring accountability and accuracy in medication management. By using this form, caregivers and medical personnel can enhance communication, reduce the risk of medication errors, and support effective healthcare outcomes.
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
| Fact Name | Description |
|---|---|
| Purpose of Form | Used to record all medications administered to a consumer within a healthcare setting, ensuring accuracy and accountability in medication management. |
| Key Information Included | Consumer's name, attending physician, month, and year, alongside a daily tracking of medication hours. |
| Medication Hour Tracking | The form lists 31 days to accommodate all months, with 24-hour tracking for adhering to various medication schedules. |
| Abbreviations Used | R for refused, D for discontinued, H for home, D for day program, and C for changed, providing a standardized method for noting medication administration circumstances. |
| Importance of Timely Recording | Staff are reminded to record at the time of administration to ensure the accuracy of the record and to maintain compliance with healthcare standards. |
| Governing Laws | While this form is widely used, specific governing laws can vary by state, including regulations around medication administration in healthcare and long-term care facilities. |
| Application Setting | Primarily utilized in long-term care facilities, hospitals, and outpatient care settings where medication administration is a regular and critical component of care. |
| Standardization and Compliance | Adhering to the form helps facilities maintain standardization in medication administration records, aligning with legal compliance and best practices in patient care. |
To ensure the safe and effective administration of medications, it is critical to accurately fill out a Medication Administration Record Sheet. This document is a comprehensive log that assists in tracking the doses administered throughout a month, making it easier to identify missed doses or medication errors. Below are straightforward steps designed to guide you through the process of completing the form.
After completing these steps, review the form to confirm that all information is correct and fully legible. Accurate completion of the Medication Administration Record Sheet is essential for coordinating care, ensuring medication safety, and facilitating communication among healthcare providers.
What is a Medication Administration Record Sheet?
A Medication Administration Record Sheet, often abbreviated as MAR, is a document that tracks all the medications prescribed and administered to a consumer within a healthcare setting or under the care of a healthcare provider. The form typically includes the consumer's name, the medication name, dosage, frequency, and the specific times at which the medications should be administered. It also contains space to record the actual administration of each dose, including any missed doses or deviations from the prescribed regimen, with specific codes such as "R" for refused, "D" for discontinued, "H" for home, "D" for day program, and "C" for changed.
Why is maintaining an accurate Medication Administration Record Sheet important?
Maintaining an accurate Medication Administration Record Sheet is crucial for several reasons, including ensuring the safety and well-being of the consumer by preventing medication errors, ensuring the correct dosage and timing of medications, and providing a clear record for healthcare providers to review. It also supports legal compliance by documenting that the care provided meets the regulatory standards.
How is a Medication Administration Record Sheet used in a healthcare setting?
In a healthcare setting, the Medication Administration Record Sheet is used by healthcare providers to document each administration of medication to a consumer. The healthcare provider checks the MAR before administering a medication to confirm the correct medication, dose, route, and time. After administration, the healthcare provider records the outcome using the designated codes and notes any relevant observations or side effects. This document serves as a communication tool between multiple caregivers to ensure continuity and consistency in medication administration.
What do the codes on the Medication Administration Record Sheet mean?
The codes on the Medication Administration Record Sheet represent different statuses for medication administration:
How often should the Medication Administration Record Sheet be updated?
The Medication Administration Record Sheet should be updated at the time of each medication administration. This real-time logging ensures the most accurate representation of the consumer's medication regimen and adherence. Any changes in medication, whether a new prescription, a discontinuation, or a change in dosage, should be promptly recorded to keep the MAR current.
What should healthcare providers do if a medication is refused or missed?
If a medication is refused by the consumer or missed for any reason, healthcare providers should record this event on the Medication Administration Record Sheet using the appropriate code (in this case, "R" for refused). They should also note the reason for the refusal or missed dose, if known, and report the incident to the supervising nurse or physician. Based on the situation, additional follow-up or intervention may be necessary to ensure the consumer's health and safety.
Can the Medication Administration Record Sheet be maintained electronically?
Yes, the Medication Administration Record Sheet can be maintained electronically. Many healthcare settings have adopted electronic health records (EHRs) that include digital versions of MARs. These systems can enhance the accuracy and efficiency of medication administration records, reduce errors associated with manual documentation, and improve communication among healthcare providers. However, it is important that digital records are kept secure and compliant with healthcare privacy laws.
What should be done when a medication is discontinued?
When a medication is discontinued, the healthcare provider should clearly mark this on the Medication Administration Record Sheet using the designated code "D" for discontinued. The date the medication was stopped should also be recorded, along with the name of the physician who made the decision. This ensures the MAR accurately reflects the consumer's current medication regimen and prevents unintentional administration of discontinued medications.
What is the role of the attending physician in regards to the Medication Administration Record Sheet?
The attending physician plays a crucial role in regards to the Medication Administration Record Sheet. They are responsible for prescribing all medications and any changes to the consumer's medication regimen, including starts, changes, and discontinuations. The physician's orders are recorded on the MAR by healthcare providers to guide the safe and accurate administration of medications. Additionally, the physician must review the MAR as part of ongoing patient care, ensuring that medication management is appropriate and responding to any issues flagged through the MAR.
How can mistakes on the Medication Administration Record Sheet be corrected?
Mistakes on the Medication Administration Record Sheet should be corrected according to the healthcare facility's policy, which often includes striking through the error with a single line, recording the correct information nearby, and initialing and dating the correction. It's important not to obliterate the original entry, as the correction process itself provides a transparent history of actions taken. All corrections should be made as soon as the mistake is noticed to ensure the record accurately reflects the medication administration activities.
When handling the Medication Administration Record Sheet, precise and accurate documentation is crucial for ensuring the safety and well-being of the individual receiving care. However, several common mistakes can occur during the completion process. Identifying and avoiding these mistakes is key to maintaining the integrity of the medication administration process.
Incorrect or Incomplete Consumer Information: Failing to accurately fill in the consumer's name, along with the month and year, can lead to serious confusion and errors in medication administration. It's vital that every sheet clearly identifies the individual it pertains to, alongside the correct period the record covers.
Omitting the Attending Physician's Name: The physician's name is crucial for verification and accountability. If there are questions or concerns about the medications listed, or if an adverse reaction occurs, healthcare providers must know which physician to contact without delay.
Misunderstanding the Abbreviations: The abbreviations (R for Refused, D for Discontinued, H for Home, and C for Changed) are critical for documenting the status of each administered medication. Misinterpretation or misuse of these abbreviations can result in inaccurate records, potentially leading to the readministration of a discontinued medication or misunderstanding about the patient's compliance.
Failure to Record at the Time of Administration: It's imperative to document the medication precisely at the time of administration. Delayed or retrospective recording can lead to inaccuracies about when (or if) the medication was actually given, affecting the medication's efficacy and the individual's health.
By paying close attention to these details, those responsible for filling out the Medication Administration Record Sheet can significantly reduce the risk of errors, ensuring that individuals receive appropriate and safe medication management.
The Medication Administration Record Sheet is a crucial document in healthcare settings, ensuring that individuals receive their medications accurately and on schedule. Accompanying this form, several other documents play vital roles in healthcare management, patient care, and compliance with regulations. These documents support the administration record by offering additional information on the patient's health status, medication directives, and care guidelines.
Together, these forms and documents create a robust framework for medication management, ensuring patient safety, effective treatment, and regulatory compliance. The Medication Administration Record Sheet, along with these complementary documents, forms a comprehensive view of a patient's medication regimen, contributing to high-quality care.
Treatment Plan: The Treatment Plan is similar to the Medication Administration Record Sheet, as both forms are essential in managing a patient's care. They document specific details about the patient's treatment, including medication details in the Medication Administration Record and broader treatment strategies in the Treatment Plan.
Patient Progress Notes: These notes are akin to the Medication Administration Record Sheet in that both track the patient's progress over time. While the Medication Administration Record focuses on medication compliance, Patient Progress Notes provide a broader view of the patient's overall journey, including responses to treatment and changes in condition.
Daily Nursing Log: Similar to the Medication Administration Record Sheet, the Daily Nursing Log documents the care provided to a patient within a 24-hour period, including medication administration, but it also covers other nursing care activities and observations.
Medical History Form: This form, while more comprehensive and encompassing a patient’s entire medical history, shares similarities with the Medication Administration Record Sheet in documenting important healthcare information. Both serve as critical tools in understanding a patient's health background for informed care decisions.
Prescription Record: A Prescription Record and the Medication Administration Record Sheet have similar functions in tracking the medications prescribed to a patient. The key difference is that the Prescription Record focuses on the doctor's orders, whereas the Medication Administration Record Sheet documents the actual administration of those orders.
Medical Orders Sheet: This sheet details a physician's orders for patient care, including medications, treatments, and interventions. It is similar to the Medication Administration Record Sheet, as both ensure that the prescribed care is accurately followed and documented.
Vaccination Record: The Vaccination Record, much like the Medication Administration Record Sheet, tracks specific healthcare interventions – in this case, vaccinations. Both are crucial for maintaining up-to-date information on a patient's medical interventions.
Pharmacy Dispensing Log: This log records medications dispensed by a pharmacy, similar to how the Medication Administration Record Sheet tracks medication administration at the point of care. Both ensure accurate medication management and accountability.
Health Monitoring Charts: Health Monitoring Charts, used to record various health parameters over time (such as blood pressure, glucose levels, etc.), are similar to the Medication Administration Record Sheet because they both play a role in tracking specific aspects of a patient's health on a regular basis.
When filling out the Medication Administration Record (MAR) Sheet, it is crucial to ensure the accuracy and completeness of the information provided. This helps in maintaining a clear and effective medication administration process. Below are important dos and don'ts to consider:
Do:Adhering to these guidelines helps ensure the safety and well-being of the consumer by reducing the risk of medication errors. Additionally, it supports healthcare providers in maintaining a consistent and legal record of medication administration.
There are several misconceptions about the Medication Administration Record (MAR) Sheet form, which is crucial for ensuring proper medication management. Clarifying these misunderstandings can help improve patient care and compliance with regulations. Here are seven common misconceptions:
Understanding these aspects of the Medication Administration Record Sheet can significantly enhance medication management practices, ensuring that patients receive the best care possible while complying with legal and regulatory standards.
When handling the Medication Administration Record Sheet, it's crucial to understand the significance of accurate and timely entries. Here are key takeaways for effectively filling out and using this form:
Consistent, accurate completion of the Medication Administration Record Sheet is essential for ensuring the safety and well-being of individuals requiring medication. It serves as a critical communication tool among healthcare providers, caregivers, and pharmacy staff. Proper use of this form can significantly reduce medication errors and enhance the overall quality of care.
Quest Diagnostics Requisition Form - The flexibility of billing options on the form ensures that patients and doctors can navigate the financial aspects of testing with ease, prioritizing health over administrative concerns.
How to Change Mailing Address - Permits postal employees to update licensure or professional certifications on file.
Letter of Permission to Travel - Provides a structured format for parents to express consent regarding their child’s NCL activity involvement.