Free Medication Count Sheet PDF Template
Free Medication Count Sheet PDF Template
In the realm of healthcare, particularly within settings such as nursing homes, residential care facilities, and hospitals, the accurate tracking of medication is crucial for patient safety and regulatory compliance. The Medication Count Sheet form serves as an essential tool in this process, offering a structured method for caregivers to document the dispensation of pharmaceuticals to residents. It encompasses several vital pieces of information including the resident's name, the quantity of medication at the start, the date and time of each administration, the drug's strength, and signatures from the administering staff. Furthermore, it meticulously tracks the quantity of medication administered and the remaining quantity, ensuring that any discrepancies can be promptly addressed. This systematic approach not only aids in the prevention of medication errors but also facilitates transparent communication among healthcare providers, and supports adherence to medication management protocols, thereby safeguarding the wellbeing of individuals under care.
|
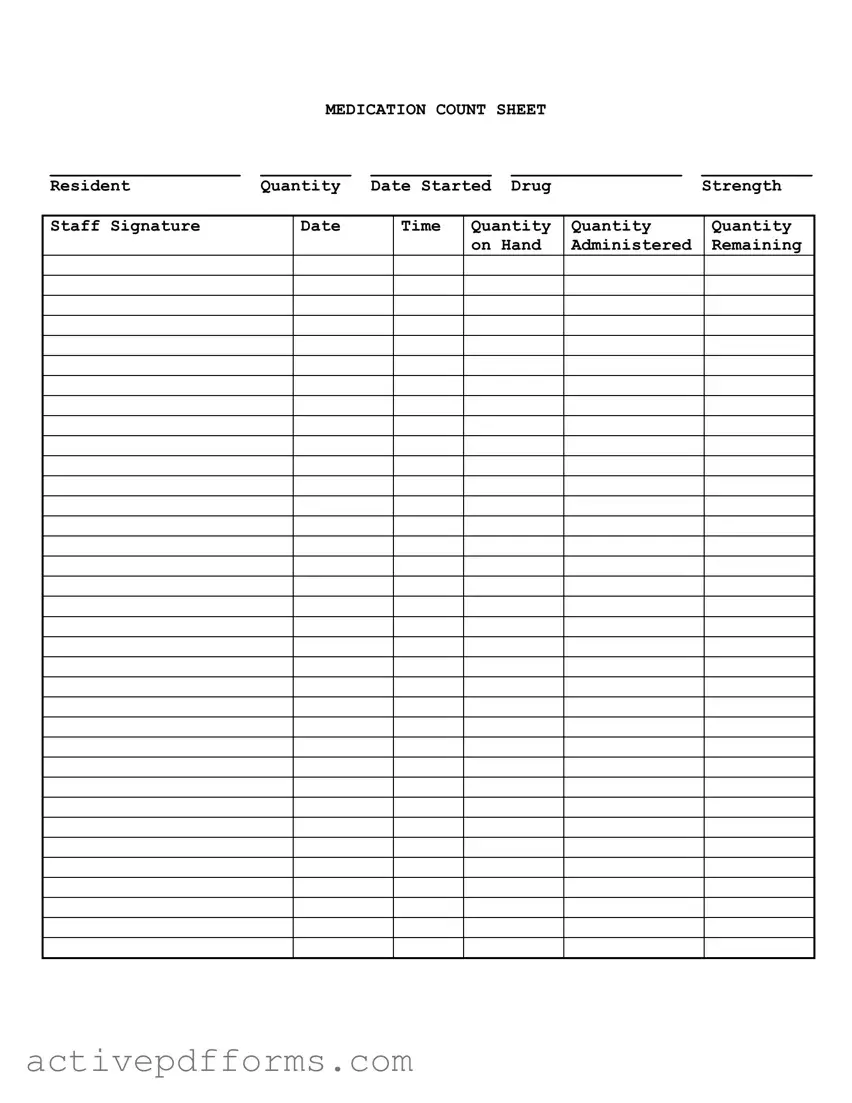
MEDICATION COUNT SHEET |
|
||
___________________ |
_________ |
____________ |
_________________ |
___________ |
Resident |
Quantity |
Date Started |
Drug |
Strength |
Staff Signature
Date
Time
Quantity |
Quantity |
Quantity |
on Hand |
Administered |
Remaining |
|
|
|
| Fact | Description |
|---|---|
| 1. Purpose | Tracks medication administration to residents, including when and how much is given. |
| 2. Key Components | Includes resident name, medication quantity, date started, drug strength, staff signature, and quantities related to administration. |
| 3. Monitoring Drug Administration | Facilitates accurate tracking of dosages administered and remaining quantities, ensuring residents receive proper care. |
| 4. User Base | Primarily used by healthcare facilities' staff responsible for administering medications. |
| 5. Legal Importance | May be governed by state-specific laws regulating the handling and documenting of medication in healthcare settings. |
| 6. Record Keeping | Essential for compliance with healthcare regulations and for providing proof of proper medication management. |
Filling out a Medication Count Sheet is a crucial task in managing the medication regimen of individuals, ensuring that the medication is administered correctly and efficiently. It serves as an official record, tracking the usage, administering of doses, and the inventory of the medications on hand. Proper completion of this form aids in maintaining accuracy in medication management, preventing errors, and ensuring the well-being of the individuals under care. To accurately fill out the Medication Count Sheet, follow these steps for a clear, error-free document.
After carefully completing each step, review the Medication Count Sheet for accuracy and clarity. This document plays a critical role in the management of medication, serving as a real-time ledger that ensures the health and safety of those under care. Accurate and diligent completion of the Medication Count Sheet is a responsibility that contributes significantly to the quality of care provided.
What is a Medication Count Sheet?
A Medication Count Sheet is a document used mainly in healthcare settings, such as assisted living or nursing homes, to track the medication administered to a resident. It records various details including the resident's name, the quantity of medication at the start, the drug name and strength, the date and time when medication is given, and the remaining quantity. Staff signatures are also included to ensure accountability.
Why is it important to maintain a Medication Count Sheet?
Maintaining a Medication Count Sheet is crucial for several reasons. It ensures that residents receive their medications correctly and at the right times, helps in preventing medication errors, and supports the accountability of healthcare staff. Additionally, it provides a reliable audit trail that can be important in the case of disputes or investigations into healthcare practices.
How should the Medication Count Sheet be filled out?
Resident Quantity: Enter the initial quantity of the medication when it first came into the facility's possession.
Date Started: Record the date when the resident began taking the medication.
Drug and Strength: List the name of the medication and its dosage strength per unit.
Staff Signature: The staff member who dispenses or administers the medication should sign their name for each entry.
Date, Time, Quantity Administered, and Quantity Remaining: These sections are filled out each time the medication is administered, noting the exact time and quantity given and the quantity left.
This precise recording helps manage medication effectively and ensures that proper procedures are followed.
What happens if a mistake is made on the Medication Count Sheet?
If a mistake is made, it is important not to erase or overwrite the incorrect information. Instead, a line should be drawn through the incorrect entry, and the correct information should be written neatly beside it or in the next available space. The staff member making the correction should initial and date the change. This process helps maintain the integrity of the sheet and provides a transparent account of what occurred and how it was rectified.
Can a digital Medication Count Sheet be used instead of a paper form?
Yes, digital Medication Count Sheets can be used and are becoming increasingly common. They offer several advantages, such as reducing the risk of lost documents, easier access for multiple staff members, and sometimes automated features that alert staff when medications need to be administered or refilled. However, it is essential to ensure that the digital system is secure, compliant with healthcare privacy laws, and has a reliable backup in case of technical issues.
One common mistake is not fully completing all sections of the form. This includes leaving blank spaces where information about the resident, medication name, dosage, or quantity should be entered. Each section helps ensure accurate tracking and accountability for medication management.
Another error is incorrectly recording the date and time medication is administered. This can lead to confusion about when the next dose is due, potentially causing medication errors such as missed or double doses.
People often miscalculate the remaining quantity of medication. Accurate calculation is crucial to monitor supply levels and determine when refills are necessary, thereby avoiding medication interruptions.
Forgetting to sign the form is a significant oversight. The staff signature verifies that the medication was administered as recorded, providing a legal and professional accountability trail.
Illegible handwriting can lead to misinterpretations of medication types, strengths, or dosages, increasing the risk of medication errors. Clear writing ensures that everyone involved in care understands the medication regimen.
Not regularly reviewing and updating the Medication Count Sheet introduces the risk of working with outdated information, especially when medication orders change.
Failure to document discrepancies between the expected and actual medication count can indicate problems such as medication mismanagement or diversion. It's vital to investigate and document any differences to maintain safety and compliance.
Using shorthand or abbreviations that are not universally understood can cause confusion. Standardizing entries by using full drug names and clear instructions ensures clarity and reduces errors.
It's essential to approach the Medication Count Sheet with care, ensuring that entries are accurate, legible, and complete. Adhering to these best practices supports effective medication management and the well-being of the individuals under care.
In a care facility or medical environment, maintaining accurate records is crucial for patient safety and compliance. The Medication Count Sheet plays a vital role in tracking the distribution and inventory of medications. However, to ensure a comprehensive approach to medication management and patient care, several other forms and documents are frequently used alongside the Medication Count Sheet. Each of these documents serves a unique purpose, contributing to the effectiveness and safety of medication administration.
Together, these documents create a framework for safe and effective medication management. They ensure that patients receive the right medications in the correct doses and at the appropriate times, while also protecting against errors and ensuring legal compliance. Utilizing these forms in conjunction with the Medication Count Sheet enhances the quality of care, supports the well-being of patients, and maintains the integrity of healthcare practices.
Inventory Control Sheet: Similar to the Medication Count Sheet, an Inventory Control Sheet tracks the quantities of items in stock, including the item name, date received or sold, and the quantity remaining. While one focuses on medication specifically, both documents serve the crucial role of monitoring resources to prevent shortages and ensure availability.
Patient Medication Profile: This document also emphasizes the importance of managing medications, listing all prescriptions a patient is taking, their dosages, and administration schedules. The connection lies in their shared goal of ensuring patient safety and medication accuracy, with the Medication Count Sheet providing a more focused view on quantities.
Daily Cash Report: At first glance, a financial document seems quite different. However, the Daily Cash Report and the Medication Count Sheet share a foundational similarity in tracking daily transactions or changes. Both detail opening amounts (or quantities), additions, subtractions, and the remaining total, ensuring accountability and accuracy in different spheres.
Treatment Administration Record (TAR): The TAR is closely related, documenting when patients receive their medications, treatments, or therapies, including the time and quantity. While the TAR focuses on the administration to patients, the Medication Count Sheet tracks inventory levels, both serving to corroborate and ensure the proper care and management of medication.
When filling out a Medication Count Sheet, accuracy and attention to detail are key. Here are some guidelines to follow:
Do:When managing medication for residents in healthcare facilities, it's crucial to understand the purpose and process of using a Medication Count Sheet form correctly. However, there are several misconceptions about this document that can affect its effective use. Here are eight common misunderstandings:
Understanding the facts about the Medication Count Sheet form can dramatically improve medication management practices, ensuring safety and compliance in healthcare settings. It's not just a regulatory requirement but a tool to safeguard the well-being of residents under care.
The Medication Count Sheet form is a crucial document in the management of a resident's medication within a care facility. Its proper use ensures not only compliance with legal and health standards but also provides a clear record of medication administration. Here are several key takeaways about filling out and using this form:
In conclusion, the conscientious use of the Medication Count Sheet form plays an essential role in the provision of safe and effective medication management in care facilities. Its proper use is a cornerstone of quality care and legal compliance, safeguarding both the well-being of residents and the integrity of the caregiving institution.
Home Health Documentation Checklist Tool - Evaluation of patient referral sheet for accuracy and timely initiation of care as per updated standards.
I9 - An asset for recruiters looking to quickly and accurately verify an applicant's employment background.